Downloaded 70 times

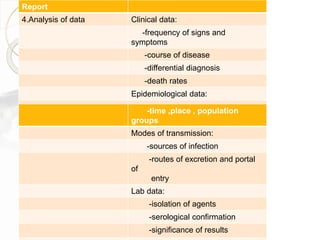
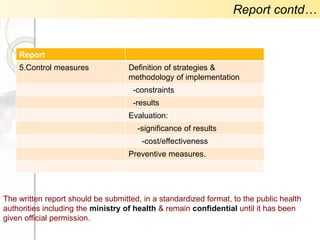
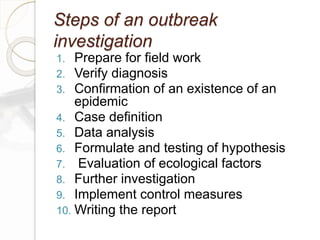
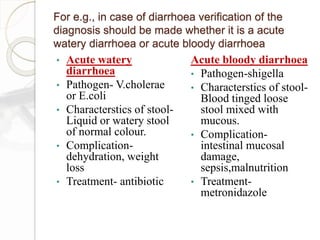
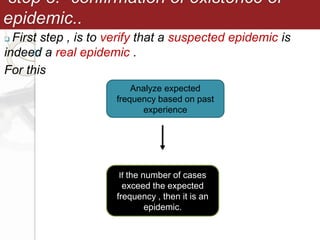











1. An investigation was conducted into an epidemic of diarrhoeal diseases to determine its scope, contributing factors, and cause. 2. The investigation aimed to define the extent of the outbreak, identify the conditions and factors responsible, and determine the source of infection and mode of transmission in order to control the epidemic. 3. Standard methods of outbreak investigation were followed, including establishing a case definition, analyzing epidemiological data on time, place, and person, formulating and testing hypotheses, and making recommendations to prevent future outbreaks.