Downloaded 11 times



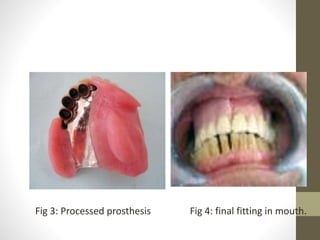
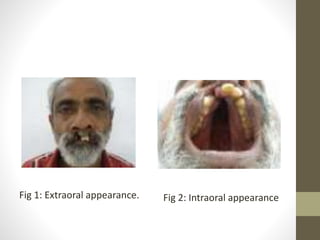
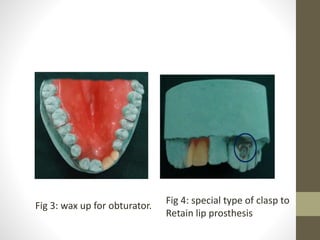
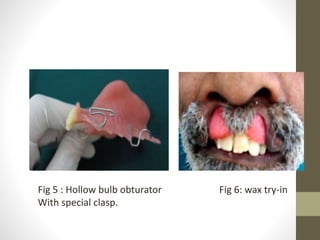
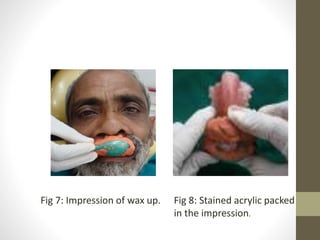

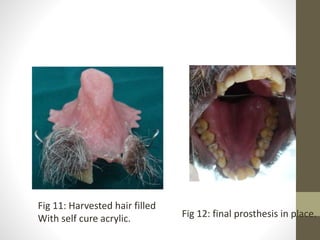
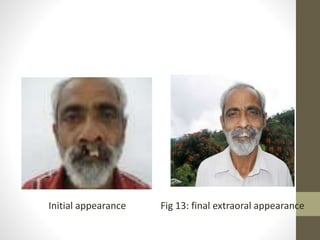

This document summarizes three case studies involving maxillofacial prosthetics: Case 1 describes a patient who underwent surgery for a fungal infection, leaving a maxillary defect that was rehabilitated with a magnet-retained facial prosthesis combined with a maxillary obturator. Case 2 involves a patient who underwent a maxillectomy for cancer treatment. His existing obturator prosthesis was failing, so precision ball attachments were added to enhance retention. Case 3 presents a patient with congenital palatal and bilateral cleft lip defects. A hybrid prosthesis was fabricated with a hollow bulb obturator and a labial extension to rehabilitate the defects.



































































