History
- Boxing isa combat sports starts in Ancient Greece and appeared in Ethiopia as early as 6000BC. In ancient
Greece, boxing was known as "pygme" or "pygmachia" (πυγμαχία), derived from "pyge" (πύγη), meaning
"fist”. In 1681 there was first recorded used of ‘boxing’ in English Literature (Richard et al. 1904). Boxing first
appeared as an Olympic sport at the Olympiad in 688 BC, but fist-fighting contests must certainly have had
their origin in mankind’s prehistory.
- The first recorded modern boxing match with gloves and rules took place in ENGLAND, James Figg vs.
Ned Sutton held on May 20, 1719, Marked the beginning of modern boxing. “Amateur Boxing Association”
was founded in England in 1880
- International Amateur Boxing Association (AIBA) was founded in 1946 in London and since then AIBA
has been the official world organization of amateur boxing. At present AIBA has 196 affiliated national
federations. (Ramin K. 2009)
3.
Introduction
• Boxing isdefined as a “a contest of fighting with fists, usually with gloved hands, in a square or circular
ring, under prescribed rules” (Oxford English Dictionary)
• Boxing: A competitive sport in which two participants engage in a contest of strength, speed, agility, and
endurance, with the objective of scoring points or knocking out their opponent. (International Boxing
Federation, 2022)
• FAMOUS ATHLETES: Mary Kom (first Indian female boxer to win a medal at the Olympics, clinching
a bronze at London 2012.), Vijender Singh Muhammad Ali, Mike Tyson
• Boxers rely on a combination of strength, coordination, velocity, and stamina to succeed in impacting the
opponent while evading adversary punches. A successful performance requires the ability to deliver
precise punches above the belt, to the head or the torso without being punched back.
• . Punching in boxing requires a combination of force and velocity of the acting arm, originating from an
optimal synchronization of the different body segments.
4.
Rules of Game
•THE FIELD OF THE PLAY
A) RING:
i. The ring must measure 6.10m inside the ropes
on all four sides.
ii. The size of apron must extend or 85cm outside
the line of the ropes on each side, including
additional canvas necessary to tighten and
secure it.
iii. The ring must have the dimensions in
accordance with the manufacturer
Guidelines: AIBA official Ring
• For the total height of the poles, distance between
the ropes and the width of the rope strips, a
margin of 2cm is accepted
5.
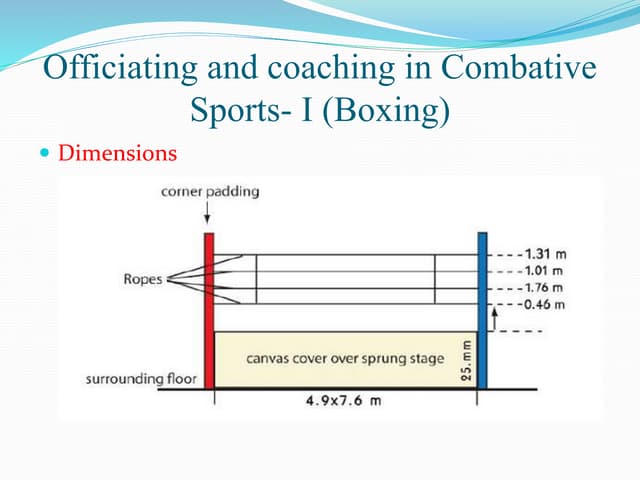
⮚ Platform andcorner pads: The platform must be 100 cm from
the ground The length and the width of the ring platform must be 7.80m x
7.80m.
• Surface of the ring floor
The floor must be covered with felt, rubber or other suitably
approved material that is soft quality and elasticity. It must not be less than 1.5 cm and no more than 2.0 cm.
• Ropes
⮚ The ropes must be covered by a thick padding.
⮚ The ring must include four (4) separate ropes on each side of the corner posts. They must be 4cm-thick,
without considering the cover.
⮚ The heights of the four (4) ropes must be 40 cm, 70 cm, 100 cm, and 130 cm from the canvas.
A) RINGSIDE ACCESSORIES
• The following ringside accessories are required for all Bouts:
⮚ Gong, Two (2) plastic receptacles which can be used for spitting., Chairs and tables
⮚ One (1) electronic stopwatch, One (1) AIBA Scoring System, One (1) microphone connected to the
loudspeaker system, First-aid supplies, One (1) stretcher
6.
A) GLOVES
⮚ Boxersmust wear red or blue gloves, as per the respective Boxer’s corner.
⮚ Boxers must put on their gloves before entering the ring
⮚ In AOB Elite and Youth Men’s Competitions:
⮚ - Ten (10) oz gloves (284grams) must be used for the Minimum Weight (46-48kg) category to
the Welterweight (67kg) category
• - Twelve (12) oz gloves (340grams) must be used for the Light Middleweight (71kg) category to
Super Heavyweight (92+ kg) category
A) HEADGUARDS:
⮚ A headguard must weigh a maximum of 450 grams (approx. 16 oz)
⮚ Headguards should come in 4 mandatory sizes
⮚ (S=Small, M=Medium, L=Large, XL Extra Large)
⮚ The padding of the headguards must respect a minimum thickness of 2-3 cm.
8.
classification
a) Age
Classification:
• -Theage of a boxer is determines using
his/her year of birth
• -Men and women boxers between the ages of
19 to 40 are categorized as ‘ELITE BOXERS’
• -Men and women boxers between the ages of
17 to 18 are categorized as ‘YOUTH BOXERS’
• -Boys and girls boxers between the ages of
15 to 16 are categorized as ‘JUNIOR
BOXERS’
• - In all Competitions related to Junior and
school-age boys and girls, as well as, in all
other younger age categories, the age range of
the participating Boxers must not be more than
2 years.
) Weight Classification
9.
DURATION AND NUMBEROF ROUNDS:
⮚ In Elite and Youth Men’s and Women’s Competitions, the Bouts must consist of three (3) rounds of three (3) minutes each.
⮚ In Junior Boys’ and Girls’ Competitions, the Bouts must consist of three (3) rounds of two (2) minutes each.
⮚ For all above listed Competitions, the rest time between rounds is one (1) minute.
⮚ The fight is controlled by a REFREE who works within the ring to judge and control the conduct of the fighters, rule on their
ability to fight safely, count knocked down fighters, and rule on fouls.
⮚ Up to three judges are typically present at ringside to score the bout
⮚ Each fighter has an assigned corner of the ring. Boxer enters into the ring from their assigned corners at the beginning of each
round and must cease fighting and return to their corner at the signal end of each round.
⮚ The opponent can be knocked out to the ground, if he doesn’t stand back up within 10 seconds and should be able to show that
he can defend himself. If opponent doesn’t show up it well be a win and will be known as ‘knock out’.
✔ KNOCK DOWN-
⮚ In the case of a Knockdown, the Referee must say “stop” and then begin an
⮚ Eight Count – count from one (1) to eight (8) – if the Boxer is fit to continue; and count from one (1) to ten (10) if the Boxer
is unfit to continue
⮚ -The Referee counts with intervals of one (1) second between the numbers and indicates each second with the hand so that
the Boxer who has been knocked down may be aware of the count.
⮚ A maximum of three (3) Eight Counts are given in one (1) round.
⮚ A ‘Technical knockout’ is possible as well and is ruled by the referee if a fighter is unable to safely continue to fight, based
10.
THE REFEREE:
Duties:
• Tobe primarily concerned for the health of both Boxers throughout the Bout
• To see that all rules and fair play are strictly observed.
• To use four (4) words of command:
• “Stop” when ordering the Boxers to stop boxing;
• “Box” when ordering the Boxers to continue boxing
• “Break” when breaking a clinch;
• “Time” when ordering the Timekeeper & Gong Operator to stop the
• time, and to order the Boxers to stop boxing.
• The Referee may touch with the hand a Boxer to stop and to break the Bout, or to separate the Boxers.
• To terminate a contest at any stage if one of the Boxers has received an injury which the Referee
decides the Boxer should not continue.
11.
• FOULS ANDMISCONDUCT:
A) Type of Fouls
⮚ Hitting
• -Below the belt (low blow), with the head, shoulder, forearm or elbow
• -With an open glove, the inside of the glove, wrist or side of the hand
• -With a kidney punch
⮚ Holding
• -holding and hitting
• -Locking the opponent’s arm or head, or pushing an arm underneath the arm of the
opponent
⮚ Pushing
• -Opponent’s face with an arm or elbow
• -The head of opponent back over the ropes
⮚ Attacking whilst holding the ropes or making any unfair use of the ropes
⮚ Ducking below the belt of opponent
⮚ Tripping, Kicking, Butting, Strangling, Pulling, Biting, Faking, Speaking
⮚ Not stepping back when ordered to break
⮚ Assaulting or behaving in an aggressive manner towards a Referee at any time..
12.
TECHNIQUES:
Punches:
1. JAB
2. CROSS
3.HOOK
iii.
4. UPPERCUT
i. Jab – A quick, straight punch thrown with the lead hand from the guard position.
ii. Cross – A powerful, straight punch thrown with the rear hand. From the guard position, the rear hand is
thrown from the chin, crossing the body and traveling towards the target in a straight line. The rear
shoulder is thrust forward and finishes just touching the outside of the chin.
Hook – A semi-circular punch thrown with the lead hand to the side of the opponent's head. From the
guard position, the elbow is drawn back with a horizontal fist (palm facing down)
iv. Uppercut – A vertical, rising punch thrown with the rear hand. From the guard position, the
torso shifts slightly to the right, the rear hand drops below the level of the opponent's chest and the
knees are bent slightly.
DEFENSE:
1) SLIPPING- Slippingis a technique used in boxing that is similar to bobbing. It Is considered one of the
four basic defensive strategies, along with blocking, holding, and clinching. It is performed by moving the
head to either side so that the opponent's punches "slip" by the boxer.
2) BOBBING- Bobbing is one of the basic strategies of defensive boxing, executed by slightly moving the
head to either side so that the opponent's punches slip by the boxer's head. The slip is used to evade swings,
jabs, and straight punches.
3) BLOCKING - blocking uses the boxer's shoulder, hands or arms as defensive tools to protect
against incoming attacks. A block generally receives a punch while a parry tends to deflect it.
4) COVER UP- Covering up is the last opportunity (other than rolling with a punch) to avoid an
incoming strike to an unprotected face or body.
5) CLINCHING- In this situation, the boxer attempts to hold or "tie up" the opponent's hands so he is unable
to throw hooks or uppercuts.
15.
• THE PHYSICS
•Basic physics tells us that punch force
is dependent on the Impulse-
Momentum relationship (the
change in momentum experienced by a
body under the action of a force is equal
to the impulse of the resultant force)
• - If you have more mass
(weight) and you can move
that mass quickly (momentum)
you’ll
• create more impulse on your
target.
• THIS IS WHY HEAVYWEIGHTS
HIT THE HARDEST!
16.
• ASSESSMENT:
• Pre-Assessment(Pre-Participation Evaluation)
- Subjective Assessment:
• 1. Medical history (previous injuries, surgeries)
• 2. Training history (experience, frequency, intensity)
• 3. Goal setting (competition goals, training objectives)
• 4. Pain or discomfort reporting
• - Objective Assessment
1. Posture analysis
2. Range of motion (ROM) assessment (shoulder, elbow, wrist, hip, knee,
ankle)
3. Muscle length testing (hamstrings, quadriceps, hip flexors)
4. Strength assessment (grip strength, shoulder rotators, core)
5. Functional movement screening (FMS)
6. Neurological screening (proprioception, balance)
7. Cardiovascular assessment (resting heart rate, blood pressure)
17.
• Specific BoxingAssessments:
1. Punching technique analysis
2. Hand and wrist alignment assessment
3. Shoulder and elbow joint mobility
4. Core stability testing
5. Footwork and agility assessment
• Outcome Measures:
6. Disability rating scales (e.g., Upper Limb Functional
Index)
7. Pain rating scales (e.g., Visual Analog Scale)
8. Functional movement screening (FMS) scores
9. Range of motion (ROM) measurements
10. Strength and power testing (e.g., grip strength, jump
height)
18.
• Form ofPre-bout Exam
• 1. Inspection of the head, eyes, ears, nose and throat for injuries can also
• be performed with attention to cranial nerve function.
• 2. Examination of the neck for motion and tenderness.
• 3. Check symmetry and tone of paracervical, shoulder, biceps, triceps,
• forearm muscles, interosseous and grip muscles.
• 4. Check the cervical nerves and coordination.
• 5. Examine the elbow, wrist and metacarpal joints. Have the boxer make a
• fist and palpate for possible metacarpal fractures or tendon injuries.
• Have him open the fist and recheck motion and for deformities.
• 6. Do a heart and lung exam.
• 7. Check for pain with rib compression.
• 8. Perform the abdominal exam looking for organomegaly, masses or
• tenderness.
• 9. A demonstration of heel and toe walking and tandem walking checks
• for lower extremity strength, balance and lumbar/sacral nerve function.
• 10. Each physician can develop his own particular routine as long as it
• covers the same basic functions and can be done quickly and
• comfortably
19.
Disqualifying
Conditions
• The examiningphysician at the annual exam or an appointed medical commission member at a tournament may declare a boxer
unfit to box for any condition which would endanger that boxer, his opponent or the officials. AIBA Medical Commission
Guidelines for disqualifying conditions are “evidence of or disclosed history of the following conditions in an annual and/or
pre- bout examination”:
• Acute and chronic infections, Severe blood dyscrasias, Sickle cell disease or
• trait, History of Hepatitis B, Hepatitis C or HIV infection, Refractive and
• intraocular surgery, cataract, retinal detachment, Myopia of more than -3.50
• dioptres, Recorded visual acuity in each eye of: uncorrected worse than
• 20/200, corrected worse than 20/60, Exposed open infected skin lesions
• Significant congenital or acquired cardiovascular and pulmonary
• abnormalities, Significant congenital or acquired musculoskeletal
• deficiencies, Unresolved post-concussion symptoms, which will need
• clearance from a neurologist, Significant psychiatric disturbances or drug
• abuse, Significant congenital or acquired intracranial mass lesions or
• bleeding, Any seizure activity within the last 3 years, Hepatomegaly,
• splenomegaly, ascites, Pregnancy, Uncontrolled diabetes mellitus or
• uncontrolled thyroid disease, Any implantable device which can alter any
• physiologic process, Women’s breast protector which protects any thing other
• that the breast protuberance itself.
20.
Injuries
⮚ The overallincidence of boxing injuries was 17.1 per 100 boxer matches. Boxing matches are unique to
sports, in that “the nature of this activity causes injury by intention rather than by accident”.
(Unterharnscheidt, F. et al. 1995) There is a strong correlation between the rate of injuries and the
fitness level.
⮚ The injuries most commonly seen are predominately to the head, face (face (including the eye, ear, nose,
and mouth), and the musculoskeletal system.
1) Musculoskeletal Injuries:
a) HAND / WRIST – The most common musculoskeletal injuries in boxing involve the hand and wrist. he
having the highest incidence. A 10-year prospective study at the U.S. Olympic Training Center during
training and competition demonstrated that upper-extremity injuries accounted for the majority of injuries
(32.9%) and that hand and wrist injuries accounted for more than half (62%) of all upper extremity
injuries.
21.
- THUMB
i) FirstMetacarpophalangeal Ulnar Collateral Ligament Tear: also known as ‘skier’s jump’ and due to
forcible abduction of the thumb and hyperextension of the MCP Joint.
ii) Assessment: - patient complain weakness of thumb index (pinch grip)
-injured thumb deviates 10 -20 degree – complete disruption of ligaments
-deviation within 10-20 degree of non-injured side – partial tear
iii) First Carpal Metacarpal Injury: This occur because of a punch connecting with hard objects, such as an
opponent’s head, fall on abducted thumb. These injuries are caused by striking the opponent’s head with
the radial side of the fist.
Two types of fracture – 1. Extra articular transverse fracture of base of first metacarpal about 1cm distal to
joint 2. Bennet’s fracture dislocation of first carpometacarpal joint – occur as a result of axial compression
when first metacarpal is driven proximally, shearing off its base. Assessment- immediate pain, swelling,
ecchymosis. Xray is done to confirm
22.
- WRIST
i) Second-FourthCarpal Metacarpal Injury: The most common site of involvement is at the second and third carpal
metacarpal regions, either alone or in combination. Although they are relatively rare. these injuries are due to
direct impact loading at the metacarpal heads. Subluxation or dislocation at the carpal metacarpal level probably
results from landing a direct blow with the wrist in slight volar flexion.
ii) Scaphoid Fractures: The boxer may or may not recall a specific episode during which the fracture
occurred. Symptoms may be very mild and indistinguishable from minor wrist sprains.
- KNUCKLE
iii) Second to Fourth Metacarpophalangeal Sagittal Band Tear: referred to as boxer's knuckle. They are due to direct
impact loading at the knuckle region. The most common location is at the second metacarpophalangeal level,
followed by the third, and less frequently, the fourth. Pathology consists of a stretch or tear of the extensor
mechanism sagittal bands. Symptoms include tenderness and swelling at the knuckle joint. If the tear is large
enough, the extensor tendon may subluxate or dislocate to the side opposite the tear.
iv) Metacarpal Fracture: Fracture of the neck or shaft of metacarpals results from axial loading against a clenched
fist. The second or third metacarpals can be involved following properly thrown punches, and the fourth and fifth
in improperly thrown punches. A direct blow with impact occurring at the prominent second or third knuckle joint
can produce this type of fracture despite the fact that the second and third metacarpals are less mobile than the
more ulnar metacarpals and are supported by the thenar eminence
23.
- SHOULDER
The shoulderis the second most common area for musculoskeletal injury in a boxer. There is a higher
incidence of shoulder injuries in the novice boxer as compared with the experienced boxer. These injuries
are musculotendinous strains, shoulder subluxations, and dislocations. Many novice boxers are exposed to
such injuries because of poor technique, insufficient glenohumeral stability, and inadequate upper-limb
strength. Most shoulder injuries involving the experienced boxer are overuse and impingement-type
injuries.
Ocular Injuries in Boxing: Blunt trauma to the globe produces ocular injury by one or a combination of
mechanisms termed coup, contrecoup, or equatorial expansion. Coup injury is the result of a direct blow
producing local injury at the point of impact. Direct blows to the globe produce local injury of the lids and
cornea, whereas blows that strike the globe from the less protected infratemporal direction affect the sclera,
ciliary body, and peripheral retina. Contrecoup injury refers to that occurring at some point distal to the site of
a direct blunt trauma. The ocular injuries resulting from a contrecoup force are due to shock waves that
originate at the site of impact and that traverse the globe, producing injury at the interface of tissue of different
densities. Injury due to blunt ocular trauma causing compression of the globe in an anteroposterior direction
with obligatory expansion along the equatorial plane is termed equatorial expansion injury. Equatorial
expansion causes traction on the peripheral retina in the region of the vitreous base, leading to a tear or
detachment of the retina.
24.
Acute Brain Injuries:
-Subdural Hematoma: Acute subdural hematomas are found in up to 75% of individuals who have died acutely as a
result of boxing injury. The subdural hematoma is due to tearing of bridging veins connecting the brain with the
superior sagittal sinus in the dura mater. Subdural hematomas are frequently associated with cerebral edema. The
boxer is typically drowsy or unconscious from the moment of impact. Occasionally, a short lucid interval may
intervene between the offending blows and onset of symptoms. Clinical signs include stupor, coma, and ipsilateral
pupillary dilatation.
- Intracerebral Hemorrhage: This injury is due to mechanical forces that cause differential movement between the
brain and skull, resulting in coup and contrecoup forces propagated through the brain. The hemorrhage may
consist of small petechiae or large clots occurring anywhere in the brain.
- Concussion: The Congress of Neurological Surgeons defines concussion as a “clinical syndrome characterized
by immediate and transient post traumatic impairment of neural function such as alteration consciousness.
- Grade I—Transient neurologic impairment without loss of consciousness lasting less
- than 10 seconds
- Grade II—Transient neurologic impairment without loss of consciousness lasting greater than 10 seconds.
- Grade III—Loss of consciousness with complete recovery in less than 2 minutes.
- Grade IV—Loss of consciousness with complete recovery taking greater than 2 minutes disturbance of vision,
or equilibrium, and so forth.