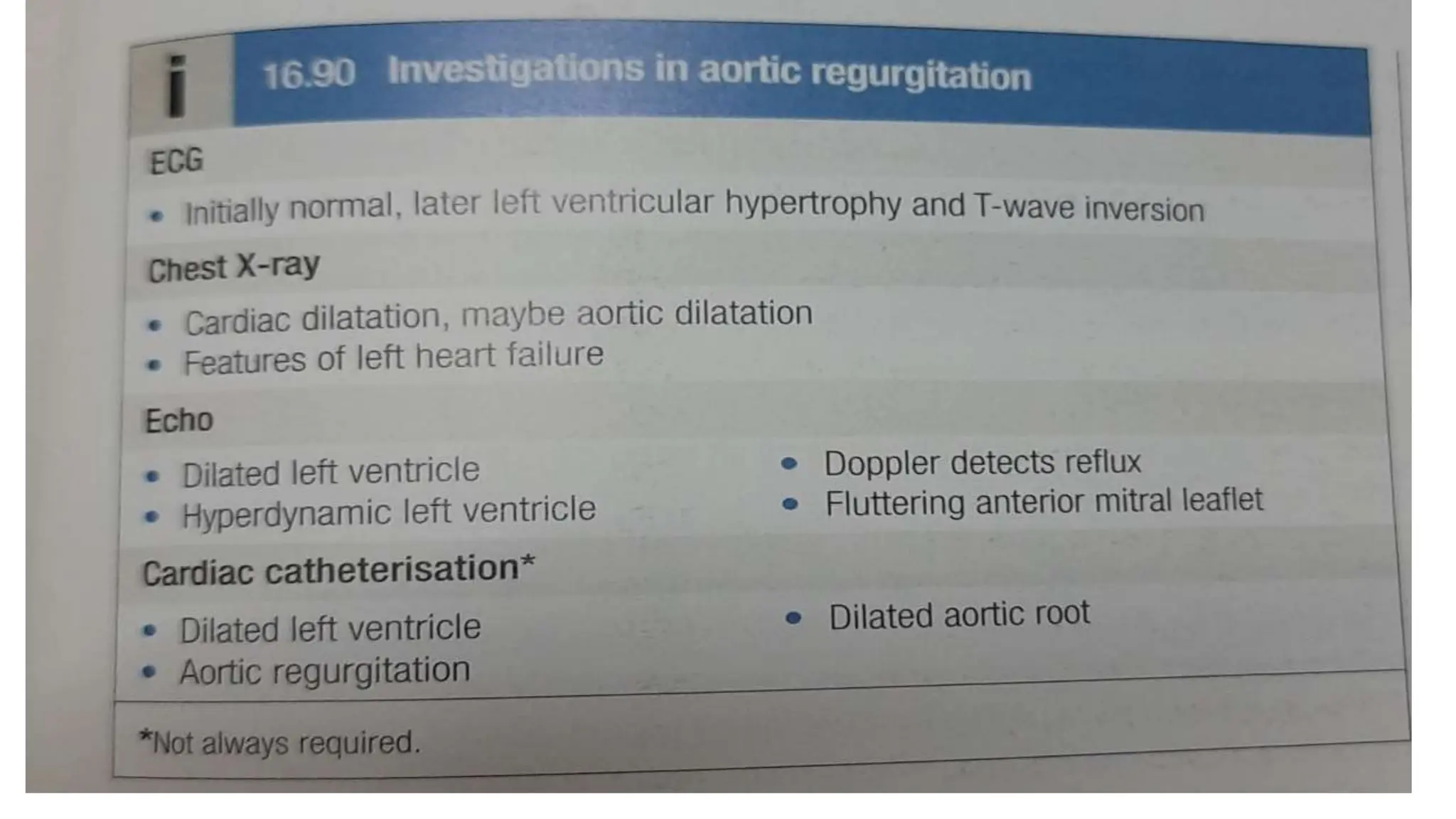
Aortic regurgitation leads to left ventricular dilation and eventual heart failure, requiring management of underlying conditions and possibly valve replacement if symptomatic. Tricuspid regurgitation presents non-specific symptoms and is identified by distinctive clinical signs, with treatment focusing on addressing right ventricular dilation and potential valve repair. Both conditions necessitate ongoing monitoring and tailored interventions based on patient symptoms and cardiac function.