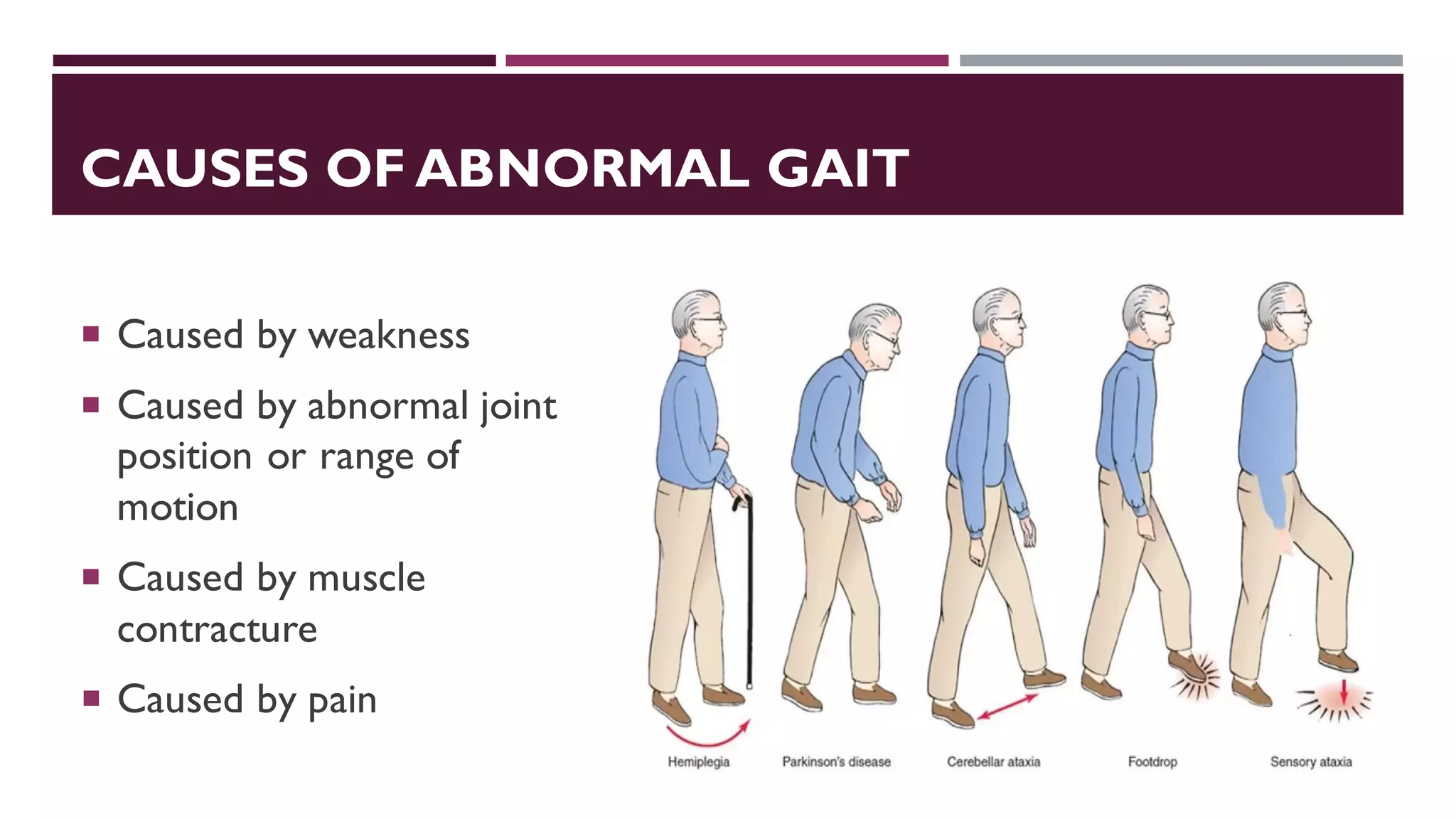
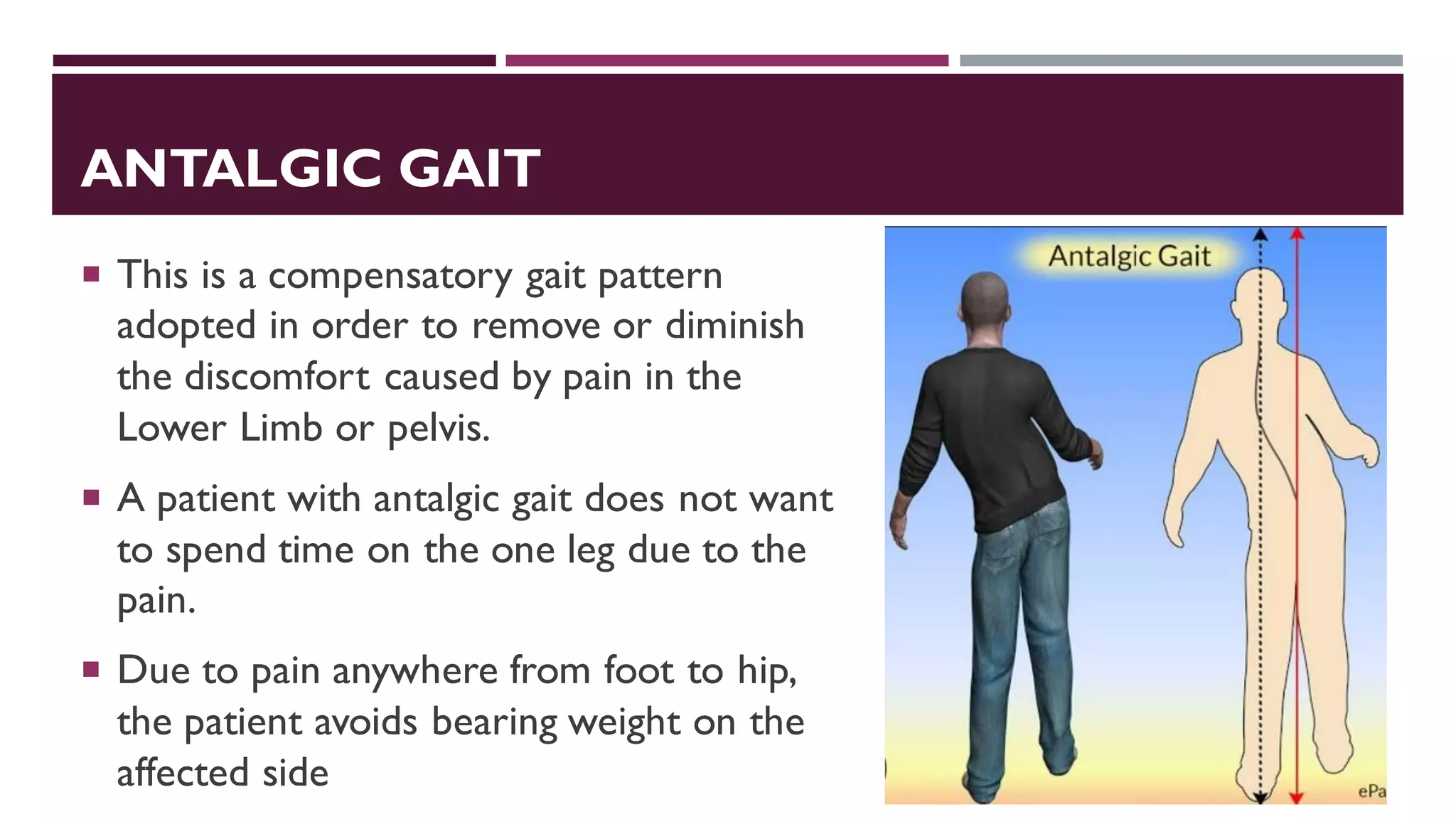
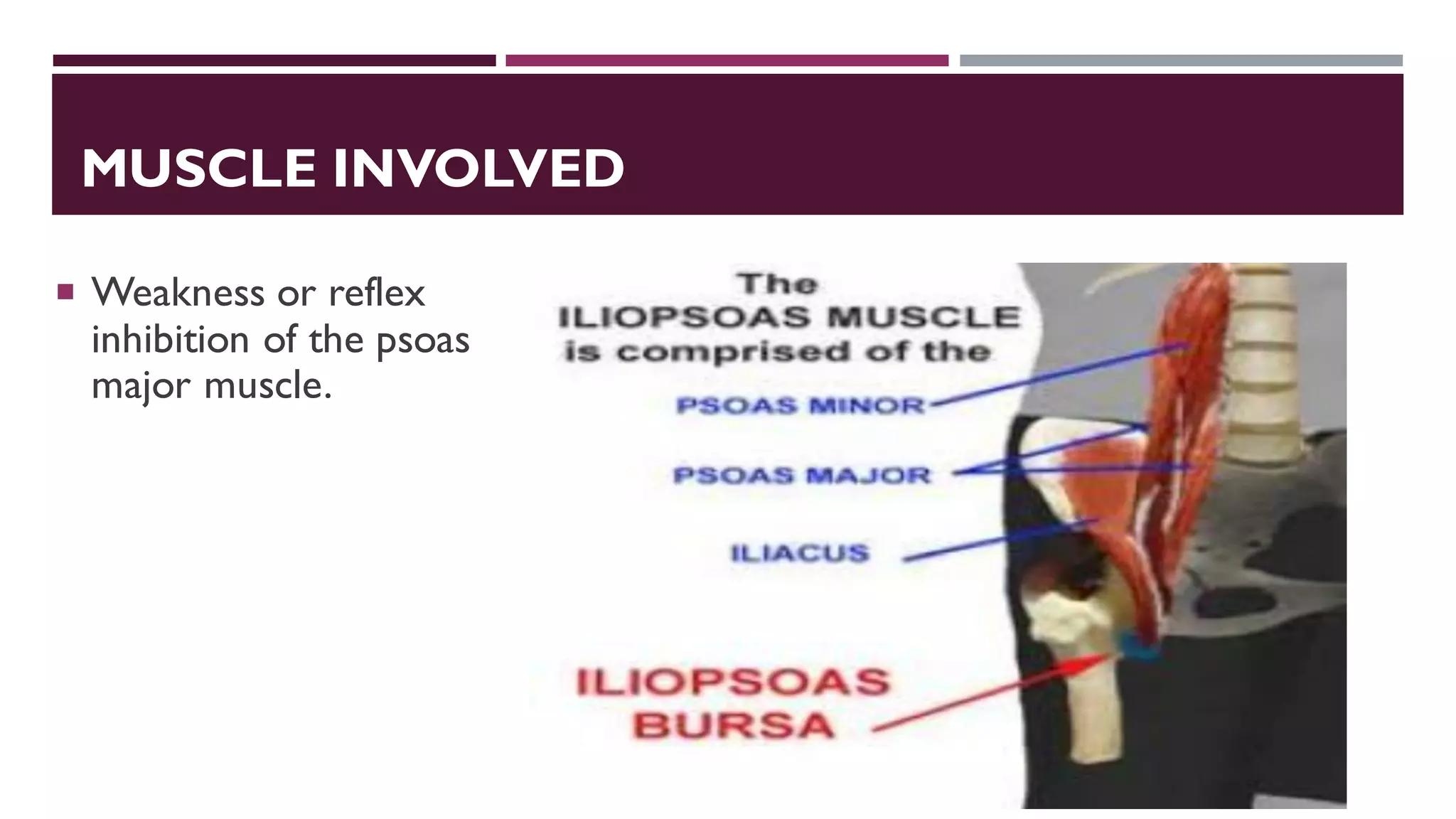
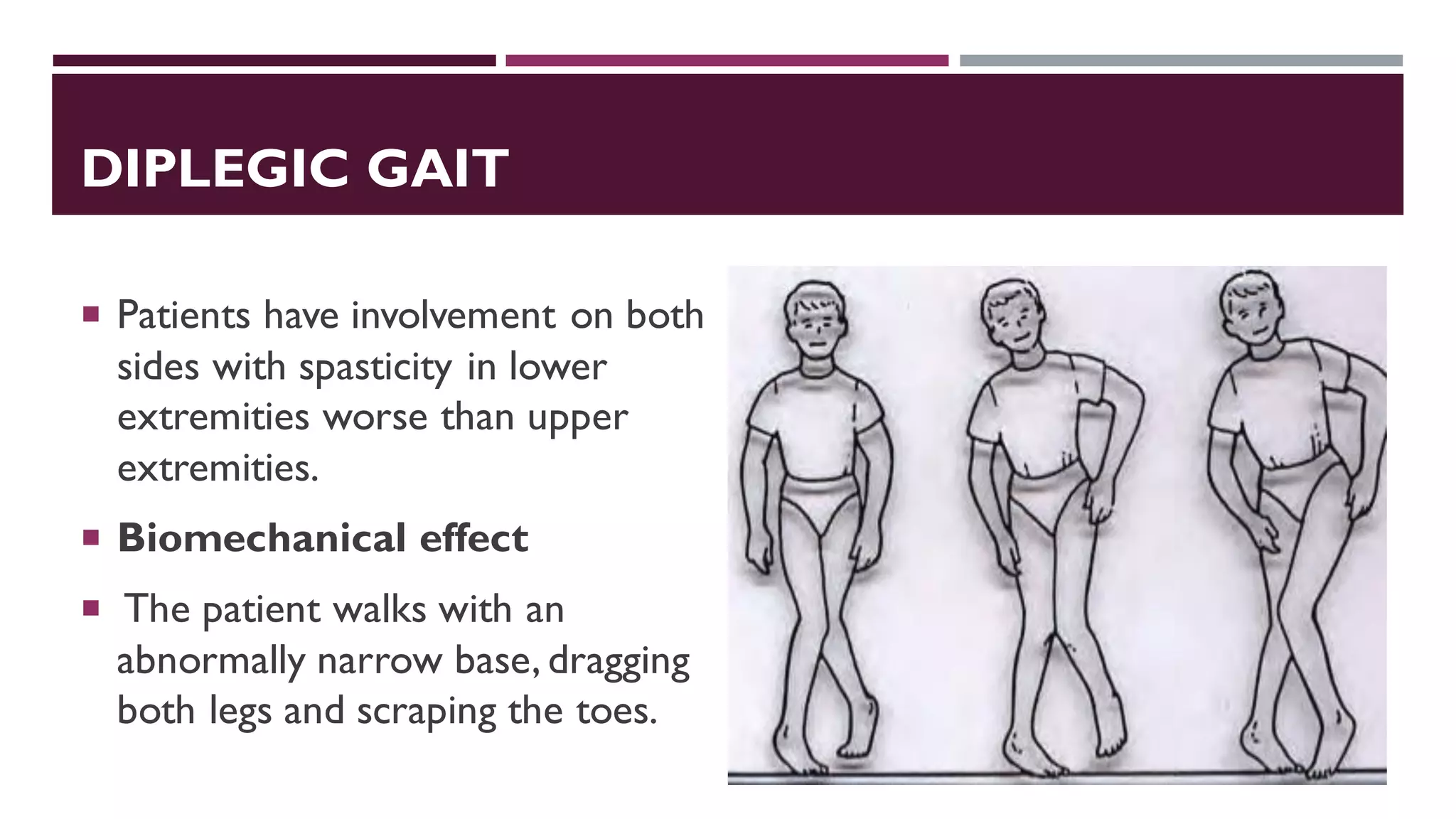
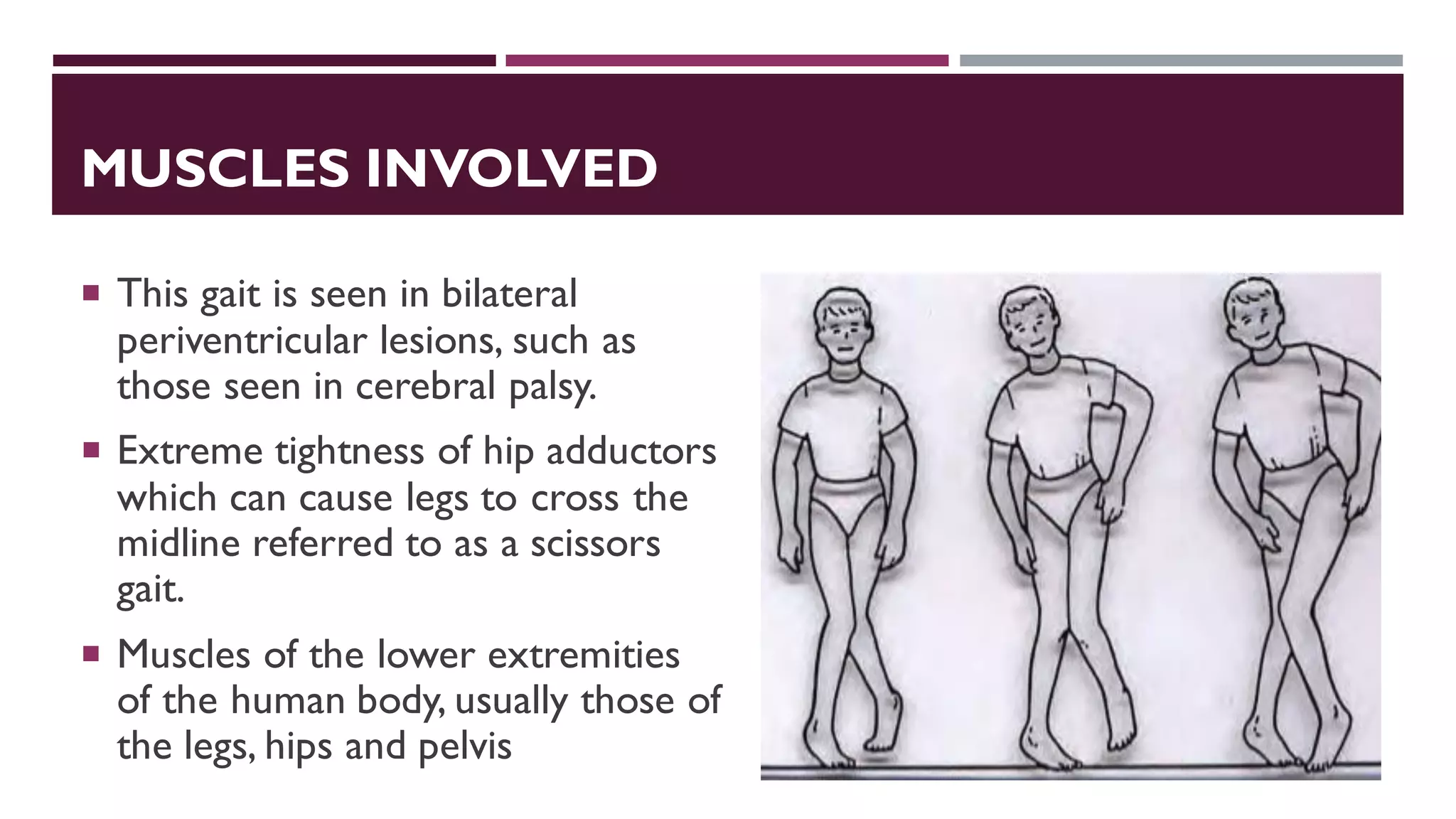
This document discusses different types of abnormal gaits caused by pain, including antalgic, gonalgic, and podalgic gaits. It focuses on antalgic gait, describing it as a compensatory walking pattern adopted to reduce pain in the lower limb or pelvis by avoiding bearing weight on the affected side. Key features of antalgic gait include shortened stance phase and enhanced swing phase on the painful side. Causes can be traumatic injuries or non-traumatic processes, and treatment involves using a cane on the opposite side. Psoatic and diplegic gaits caused by specific muscle weaknesses or injuries are also summarized.