Medical Surgical NursingI
Unit III: Perioperative Care
Pre, Intra and Post
operative nursing care
3.
Caring for perioperativeclients
Contents Outline
1.Objectives.
2.Introduction.
3.Phases of perioperative care.
4.Types of surgery.
5.Categories of surgery based on urgency.
6.Preoperative assessment.
7.Surgical risk factors.
8.Preoperative preparation.
9.Nursing diagnosis and intervention in preoperative phase.
10.Postoperative care.
11.Nursing diagnosis and intervention in postoperative period.
12.Postoperative complications.
4.
Objectives:
At the endof this lecture, the student must be able to:
•Differentiate the phases of perioperative care.
•Define the types and categories of surgery.
•Identify the preoperative assessments.
•Develop a preoperative teaching plan.
•Identify surgical risk factors.
•Describe the preoperative preparation.
•Discuss assessments needed in immediate and later postoperative
period.
•Identify the postoperative complications.
Caring for perioperative clients
5.
What is meantby
perioperative?
Perioperative is a term used to
describe the entire span of surgery,
including what occurs before,
during, and after the actual
operation.
6.
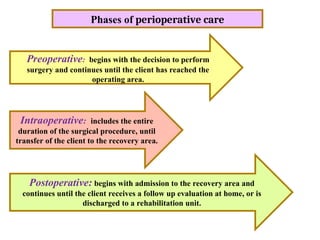
Phases of perioperativecare
Preoperative: begins with the decision to perform
surgery and continues until the client has reached the
operating area.
Intraoperative: includes the entire
duration of the surgical procedure, until
transfer of the client to the recovery area.
Postoperative: begins with admission to the recovery area and
continues until the client receives a follow up evaluation at home, or is
discharged to a rehabilitation unit.
7.
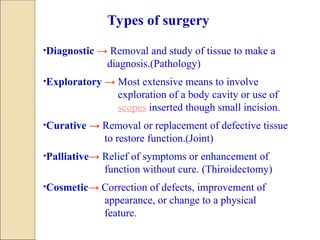
•Diagnostic → Removaland study of tissue to make a
diagnosis.(Pathology)
•Exploratory → Most extensive means to involve
exploration of a body cavity or use of
scopes inserted though small incision.
•Curative → Removal or replacement of defective tissue
to restore function.(Joint)
•Palliative→ Relief of symptoms or enhancement of
function without cure. (Thiroidectomy)
•Cosmetic→ Correction of defects, improvement of
appearance, or change to a physical
feature.
Types of surgery
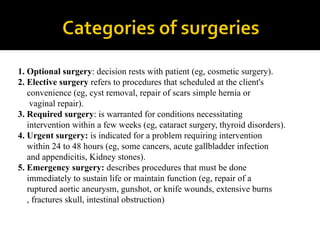
1. Optional surgery:decision rests with patient (eg, cosmetic surgery).
2. Elective surgery refers to procedures that scheduled at the client's
convenience (eg, cyst removal, repair of scars simple hernia or
vaginal repair).
3. Required surgery: is warranted for conditions necessitating
intervention within a few weeks (eg, cataract surgery, thyroid disorders).
4. Urgent surgery: is indicated for a problem requiring intervention
within 24 to 48 hours (eg, some cancers, acute gallbladder infection
and appendicitis, Kidney stones).
5. Emergency surgery: describes procedures that must be done
immediately to sustain life or maintain function (eg, repair of a
ruptured aortic aneurysm, gunshot, or knife wounds, extensive burns
, fractures skull, intestinal obstruction)
10.
CONDUCT ANURSING ASSESSMENT
PROVIDE PREOPERATIVE TEACHING
PERFORM METHODS OF PHYSICAL
PREPARATION
ADMINISTER MEDICATIONS
ASSIST WITH PSYCHOSOCIAL
PREPARATION
COMPLETE THE SURGICAL CHECKLIST
11.
:
Preoperative Assessment
I. Reviewpreoperative laboratory and
diagnostic studies
II. Review the client’s health history and
preparation for surgery
III. Assess physical needs
IV. Assess psychological needs
V. Assess cultural needs
12.
I. Review preoperativelaboratory and diagnostic studies:
•Complete blood count.
•Blood type and cross match.
•Serum electrolytes.
•Urinalysis.
•Chest X-rays.
•Electrocardiogram.
•Other tests related to procedure or client’s medical condition, such
as: prothrombin time, partial thromboplastin time, blood urea
nitrogen, creatinine, and other radiographic studies.
13.
II. Review theclient’s health history and preparation for surgery:
•History of present illness and reason for surgery
•Past medical history
•Medical conditions (acute and chronic)
•Previous hospitalization and surgeries
•History of any past problem with anesthesia
•Allergies
•Present medications
•Substance use: alcohol, tobacco, street drugs
•Review of system
14.
III. Assess physicalneeds:
•Ability to communicate
•Vital signs
•Level of consciousness
Confusion
Drowsiness
Unresponsiveness
•Weight and height
•Skin integrity
•Ability to move/ ambulate
•Level of exercise
•Prostheses
•Circulatory status
15.
IV. Assess psychologicalneeds:
•Emotional state
•Level of understanding of surgical procedure, preoperative and
postoperative instruction
•Coping strategies
•Support system
•Roles and responsibilities
V. Assess cultural needs:
•Language-need for interpreter
16.
INFORMED CONSENT
Beforesurgery, the client must sign a surgical consent form or
operative permit.
Clients must sign a consent form for any procedure that requires
anesthesia and has risks of complications.
If an adult client is confused, unconscious, a family member or
guardian must sign the consent form.
If the client is younger than 18 years of age, a parent or legal
guardian must sign the consent form.
In an emergency, the surgeon may have to operate without
consent, health care personnel, however, makes every effort to
obtain consent by telephone, or fax.
Each nurse must be familiar with agency policies and state laws
regarding surgical consent forms.
Clients must sign the consent form before receiving any
preoperative sedatives.
The nurse is responsible for ensuring that all necessary parties
have signed the consent form and that it is in the client’s chart
before the client goes to the operating room (OR).
17.
Preoperative medication-when they are given
and their effects.
Post operative pain control.
Explanation and description of the post
anesthesia recovery room or post surgical area.
Discussion of the frequency of assessing vital
signs and use of monitoring equipment.
Explanation and demonstration deep breathing
and coughing exercises, use of incentive
spirometry, how to support the incision for
breathing exercises and moving, position
changes, and feet and leg exercises.
18.
Information aboutintravenous (IV) fluids and
other lines and tubes such as nasogastric tubes.
Preoperative teaching time also gives the client
the chance to express any anxieties and fears
and for the nurse to provide explanations that
will help alleviate those fears.
When clients are admitted for emergency
surgery, time for explanation is unavailable;
explanations will be more complete during the
postoperative period.
19.
Deep breathingis a form of controlled ventilation that
opens and fills small air passages in the lungs to
prevent atelectasis and pneumonia.
Coughing is a natural method of clearing secretions
from the airways.
Leg exercises help promote circulation and reduce the
risk of forming a thrombus in the veins.
Antiembolism stockings help prevent thrombi and
emboli by compressing superficial veins and
capillaries redirecting blood to larger and deeper veins,
where it flows more effectively toward the heart.
22.
ANTICHOLINERGICS: Glycopyrrolate(robinal)
decreases respiratory secretions.
ANTIANXIETY: Lorazepam (ativan) reduces anxiety.
HISTAMINE-2 RECEPTOR ANTAGONIST:
Cimetidine (tagamet) decreases gastric acidity and
volume.
NARCOTICS: Demerol (meperidine) decreases the
amount of anesthesia needed to sedate the client.
SEDATIVES: Midazolam (versed) promotes sleep or
conscious sedation and decrease anxiety.
ANTIBIOTICS: Kanamycin (Kantrex) destroy enteric
microorganisms.
23.
History andphysical examination.
Name of procedure on surgical consent.
Signed surgical consent.
Laboratory results.
Client is wearing an identification bracelet.
Allergies have been identified.
NPO.
Skin preparation completed.
Vital signs assessed.
24.
Jewelry removed.
Dentures removed.
Client is wearing a hospital gown and hair cover.
Client has urinated.
Location of IV site, type of intravenous solution,
rate of infusion is identified.
The prescribed preoperative medication has been
given.
26.
Surgical Risk Factors:
Age Very young – Elderly
→
Nutritional Status Malnourished – Low weight –
→
Obese
Medical Problems Acute and chronic respiratory
→
problems – Hypertension – Liver dysfunction – Renal
failure – Diabetes
28.
Physical Preparation.
Skin preparation
Elimination
Food and fluids
Care of valuables
clothing/ grooming
Prostheses
Psychosocial Preparation.
Careful preoperative teaching can reduce
fear and anxiety of the clients.
29.
Nursing Diagnosis
• Anxietyrelated to results of surgery and
postoperative pain.
• Knowledge deficit related to preoperative
procedures and postoperative expectations.
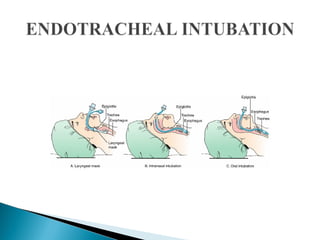
1. General Anesthesia(inhaled or intravenously) refers
to drug – induced depression of the central nervous
system that produces analgesia, amnesia and
unconsciousness (affects whole body).
2. Regional anesthesia is a form of local anesthesia that
suspends sensation and motion in body region or part;
the client remains awake. Continuous monitoring is
required in the event the block is not totally effective
and the client experiences pain or reactions to
blocking agents (e.g. nausea, cardiovascular collapse).
Regional anesthesia differs in terms of location and
size of the anatomic area anesthetized and the volume
and type of anesthesia agent used.
32.
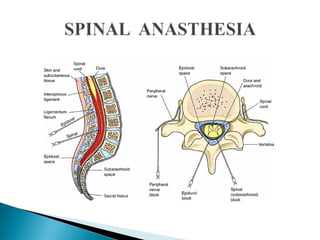
3. Spinal Anesthesiais local anesthesia injected into the
subarachniod space at lumbar level to block nerves
and suspend sensation and motion to the lower
extremities, perineum, and lower abdomen.
4. Conduction Blocks suspend sensation and motion on
various groups of nerves such as epidural block (i.e.
anesthetic into space around the dura mater); Para
vertebral block (i.e. produces anesthesia of the chest,
abdominal wall and extremities) and Tran sacral
(caudal) block (i.e. anesthesia of the perineum).
34.
◦ Surgeon performsthe surgical procedure and heads the surgical team.
◦ An anesthesiologist or anesthetist makes a preoperative assessment to
plan the type of anesthetic to be administered and to evaluate the
client's physical status.
◦ Circulating nurse manages the operating room and protects the
patient’s safety and health by monitoring the activities of the surgical
team, checking the operating room conditions, and continually
assessing the patient for signs of injury and implementing appropriate
interventions. Verify consent, ensure cleanliness, proper temperature,
humidity, and lighting; the safe functioning of equipments; and the
availability of supplies and materials.
◦ Scrubbing nurse setting up the sterile tables; preparing sutures, and
special equipments; and assisting the surgeon and the surgical
assistants during the procedure by anticipating the instruments that
will be required.
◦ Scrub nurse and circulatory nurse count all needles, sponges; and
instruments used.
35.
Verifying consent
Coordinating the team
Ensuring cleanliness, proper temp., humidity &
lighting
Safe functioning of equipment
Availability of supplies and materials
36.
Performing asurgical hand scrub
Setting up the sterile tables
Preparing sutures, ligatures & special
equipment
Assisting the surgeon during the procedure
39.
Physiologic status(LOC)
Psychosocial status (anxiety level, coping
mechanisms)
Physical status (surgical site, skin condition,
immobile joints)
40.
1. Ask thepatient about any known allergies.
2. Verify patient identification and that the correct surgery is scheduled.
3. Antidotal supplies (of anesthesia) must be available in an emergency
room.
4. Promote measures that ensure adequate tissue perfusion:
Assess the patient's vital signs continuously, respiratory status,
peripheral vascular status, and cardiovascular status.
Assist with mechanical ventilation.
5. Promote measures that maintain adequate fluid and electrolyte balance:
◦ a. Monitor intake and output accurately.
◦ b. Assess for skin turgor and mucous membranes (sings of
dehydration) nd circulatory overload (breath sounds, peripheral
edema, & jugular vein distention).
41.
6. Promotemeasures that maintain the patient's normal temperature:
◦ a. Ensure that OR temperature is between 25°C and 26.6°C.
◦ b. Warm all intravenous and irrigating solutions.
◦ c. Monitor the patient's temperature continuously.
◦ d. Remove all wet gowns and drapes promptly and replace
with dry to prevent heat loss.
7. Promote measures that decrease risk of infection:
◦ a. Maintain sterile procedures and techniques during surgery.
◦ b. Apply sterile dressings to all wounds.
◦ c. Non-scrubbed personnel refrain from touching or
contaminating anything that is sterile.
42.
8. Ensurepatient's safety in the OR:
◦ a. Remove any potential contaminants.
◦ b. Recheck electrical equipment for proper operation.
◦ c. Make sure that necessary equipment and supplies are available.
◦ d. Count and record sutures, needles, instruments, and sponges.
◦ e. Assist in transferring the patient to the OR table.
◦ f. Cover the patient with a warm blanket, and attach the safety belt.
◦ g. Remain at the patient's side during anesthesia induction.
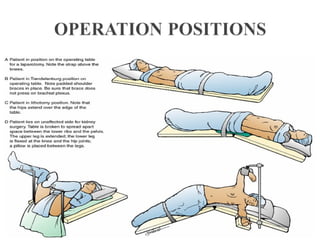
◦ h. Verify proper patient positioning to protect nerves, circulation, respiration, and
skin.
◦ i. Ensure that newly requested items are quickly supplied to the anesthesia or
scrub team by the circulating nurse.
Postoperative Care:
Postoperative Care:
Immediatepostoperative period.
Immediate postoperative period.
Initial Assessment
Airway patency
Effectiveness of respiration
Presence of artificial airways
Mechanical ventilation, or supplemental oxygen
Circulatory status, vital signs
Wound condition, including dressings and drains
Fluid balance, including IV fluids, output from catheters
and drains and ability to void
Level of consciousness and pain
46.
Postoperative Care:
Postoperative Care:
Laterpostoperative period
Later postoperative period
Ongoing Assessment
Respiratory function
General condition
Vital signs
Cardiovascular function
Fluid status
Pain level
Bowel and urinary elimination
Dressings, tubes, drains, and IV lines
47.
Immediate Postoperative care:
ImmediatePostoperative care:
Recovery Room
Recovery Room
Assess and provide intervention for the following at least 15
minutes:
1. Airway (Maintain Airway patency and optimal respiratory
function).
2. Vital signs (every 5 minutes for 3 times then every15 minute).
3. General appearance, Level of consciousness (LOC), and
movement of extremities.
4. Pain level (administers medication).
5. Urine output, drain or catheter patency.
6. Intravenous or central line patency.
7. Observe operative site, dressing, and drainage for
haemorrhage.
8. Function of cardiac and oxygen
48.
Later Postoperative care(in
Later Postoperative care (in
department):
department):
1. Assess the patient's level of consciousness.
2. Place the patient in a safe position on the side with face down
& neck slightly extended (prevents aspiration of vomitus &
airway obstruc
tion).
3. Monitor vital signs:
a. Every 15 minutes the first hour.
b. Every 30 minutes the next 2 hours.
c. Every hour for next 4 hours.
d. Finally, every 4 hours.
4. Prevents or assist with the treatment of shock
5. Maintains proper position and function of drain tubes and IV
infusion
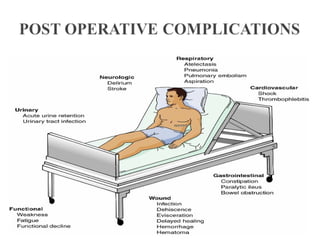
6. Monitor for potential complications
49.
When caring forpost-surgical patient, think
When caring for post-surgical patient, think
of the “4 W’s
of the “4 W’s”
”
1. Wind: prevent respiratory
complications
2. Wound: prevent infection
3. Water: monitor I & O
4. Walk: prevent thrombophlebitis
50.
Nursing Diagnosis
• Riskfor altered respiratory function related to
immobility, effects of anesthesia, analgesics and pain.
• Pain related to surgical incision and manipulation of
body structures.
• Altered Comfort (nausea and vomiting) related to
effects of anesthesia or side effects of narcotics.
• Risk for Infection related to break in skin integrity
(surgical incision, wound drainage devices).
• Activity Intolerance related to decreased mobility and
weakness secondary to anesthesia and surgery.
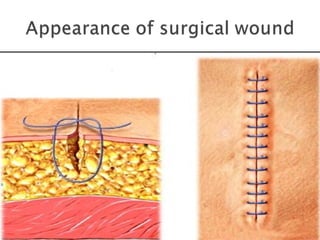
CARE OFTHE INCISION.
SIGNS OF COMPLICATIONS.
DRUGS FOR PAIN MANAGEMENT.
HOW TO SELF ADMINISTER PRESCRIBED
MEDICATIONS.
ACTIVITY LEVEL.
AMOUNT OF WEIGHT THAT CAN BE LIFTED.
DIET.
RETURN FOR A MEDICAL APPOINTMENT.