The document outlines the Enhanced Recovery After Surgery (ERAS) protocol. ERAS aims to reduce surgical stress, accelerate recovery through a multimodal approach. Key elements of ERAS include pre-admission counseling and nutrition optimization, minimizing preoperative fasting through carbohydrate loading, selective bowel preparation if needed, thoracic epidural anesthesia, early feeding and mobilization, and multimodal pain control to avoid opioid use and ileus. The goal is to minimize length of stay through evidence-based perioperative optimization.
![Back To The Past
PREOPERATIVE PROLONG FASTING
MECHANICAL BOWEL PREPARATION
NASOGASTRIC TUBE
DRAIN TUBE, [ in any GIT surgery ]
PROLONG BED REST](https://image.slidesharecdn.com/erasprotocol3-200130193949/85/Eras-protocol-3-2-320.jpg)
![Evolution of Surgical Principles replaces the dogma
and brought the concept of
THIS CONCEPT WAS FIRST
DESCRIBED BY Dr Henrik Kehlet [1990]
E R A S](https://image.slidesharecdn.com/erasprotocol3-200130193949/85/Eras-protocol-3-3-320.jpg)

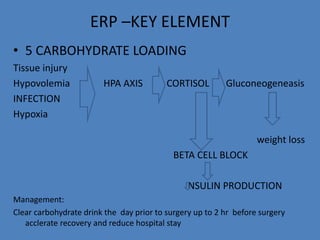
![ERP –KEY ELEMENT
2. Pre operative nutrition
In adequate nutrition independly increase risk and hospital stay
ESPN criteria[european society of parenteral and enteral nutrition] of severe
nutritional risk
weight loss> 10-15%.
BMI <18.5
Serum Albumin<30 gm/lit
MANAGEMENT:
Appropriate input
Standerd whole protein liquid nutritional
supplement](https://image.slidesharecdn.com/erasprotocol3-200130193949/85/Eras-protocol-3-9-320.jpg)
![ERP –KEY ELEMENT
• AVOID Drain tube
increases hospital stay
increase risk of infection
PREVENTION OF PONV[POST OP NAUSEA & VOMITING]
ONDENSATRON](https://image.slidesharecdn.com/erasprotocol3-200130193949/85/Eras-protocol-3-17-320.jpg)