Downloaded 28 times
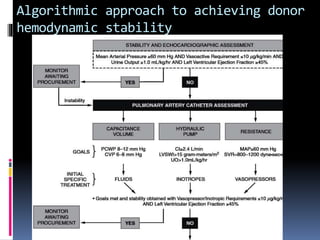
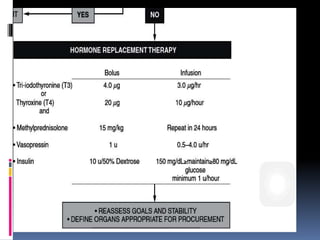
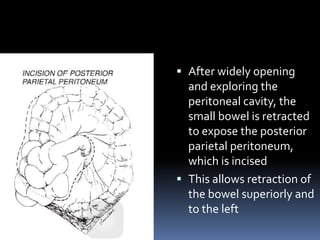
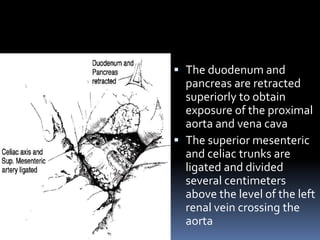
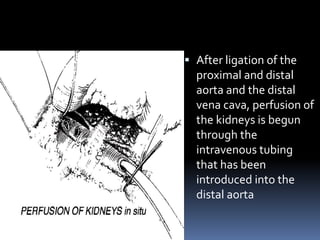
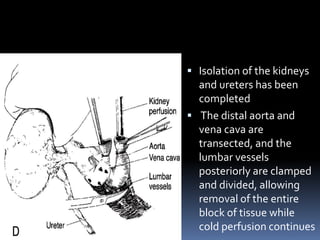
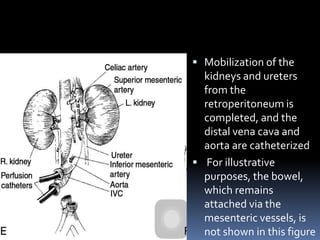
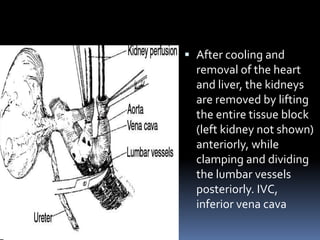

This document provides information on the prerequisites and techniques for cadaver kidney retrieval. It discusses: (1) The need to maximize the use of the existing organ donor pool by standardizing the donor management process from identification through organ retrieval. (2) The technique for cadaver donor nephrectomy without other organ retrieval, which involves opening the peritoneal cavity, ligating vessels, and perfusing and removing the kidneys while maintaining cold perfusion. (3) The technique for cadaver donor multiple organ retrieval, which involves a long incision to access the chest and abdominal cavities and sequentially retrieving organs like the heart, liver, kidneys, and pancreas after cannulating vessels and dividing connections























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
