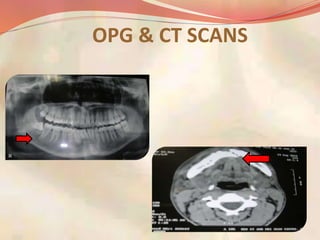
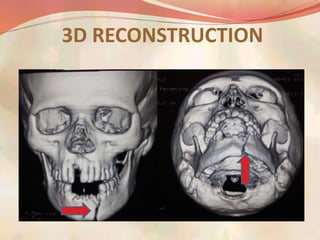
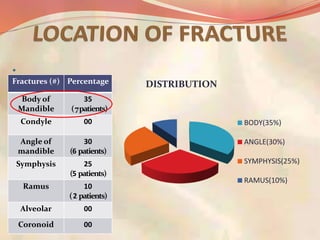
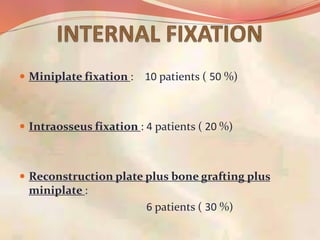
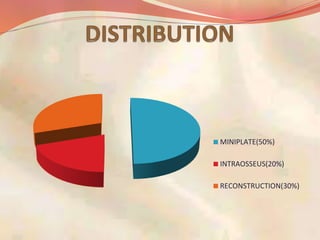
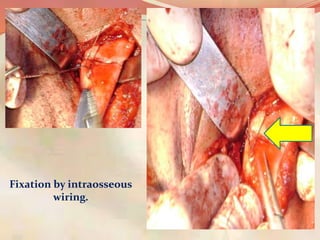
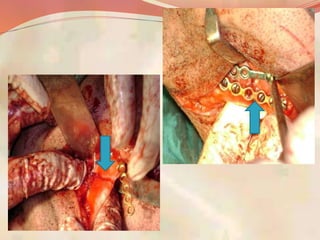
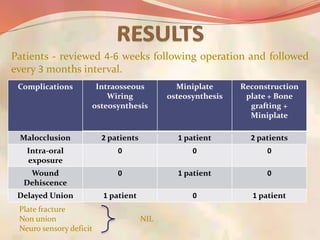
This document summarizes a study of 20 patients treated for isolated mandibular fractures over one year. The majority of fractures were in the body of the mandible. Patients were treated with miniplate fixation, intraosseous wiring, or reconstruction plating with bone grafting and miniplates. Outcomes were generally good with miniplate fixation showing fewer complications like malocclusion or delayed union compared to other methods. The study concluded that miniplate osteosynthesis provides rigid fixation and good long-term results for displaced mandibular fractures.