
Download as PDF, PPTX
![Melituria
sugar in the urine; specific types are named for the sugar in question
,such as FRUCTOSURIA, GALACTOSURIA, GLYCOSURIA, and LACTOSURIA.
Fructosuria: the presence of fructose in the urine.
Essential fructosuria a benign, autosomal recessive disorder of carbohydrat
e metabolism due to a defect infructokinase and manifested only by fructose i
n the blood and urine.
Excretion of lactose (milk sugar) in the urine; a common finding during pre
gnancy and lactation, and in new borns, especially premature babies.
Lactosuria: [lak″to-su´re-ah] elevated levels of lactose, as seen in lactose
intolerance or during lactation.](https://image.slidesharecdn.com/prabhakarsingh-ivsem-paperunitidisordersofcarbohydratemetabolism-partfirst-200520080540/75/Prabhakar-Singh-IV_SEM-Paper_Unit-I-Disorders-of-carbohydrate-metabolism-Part-First-30-2048.jpg)

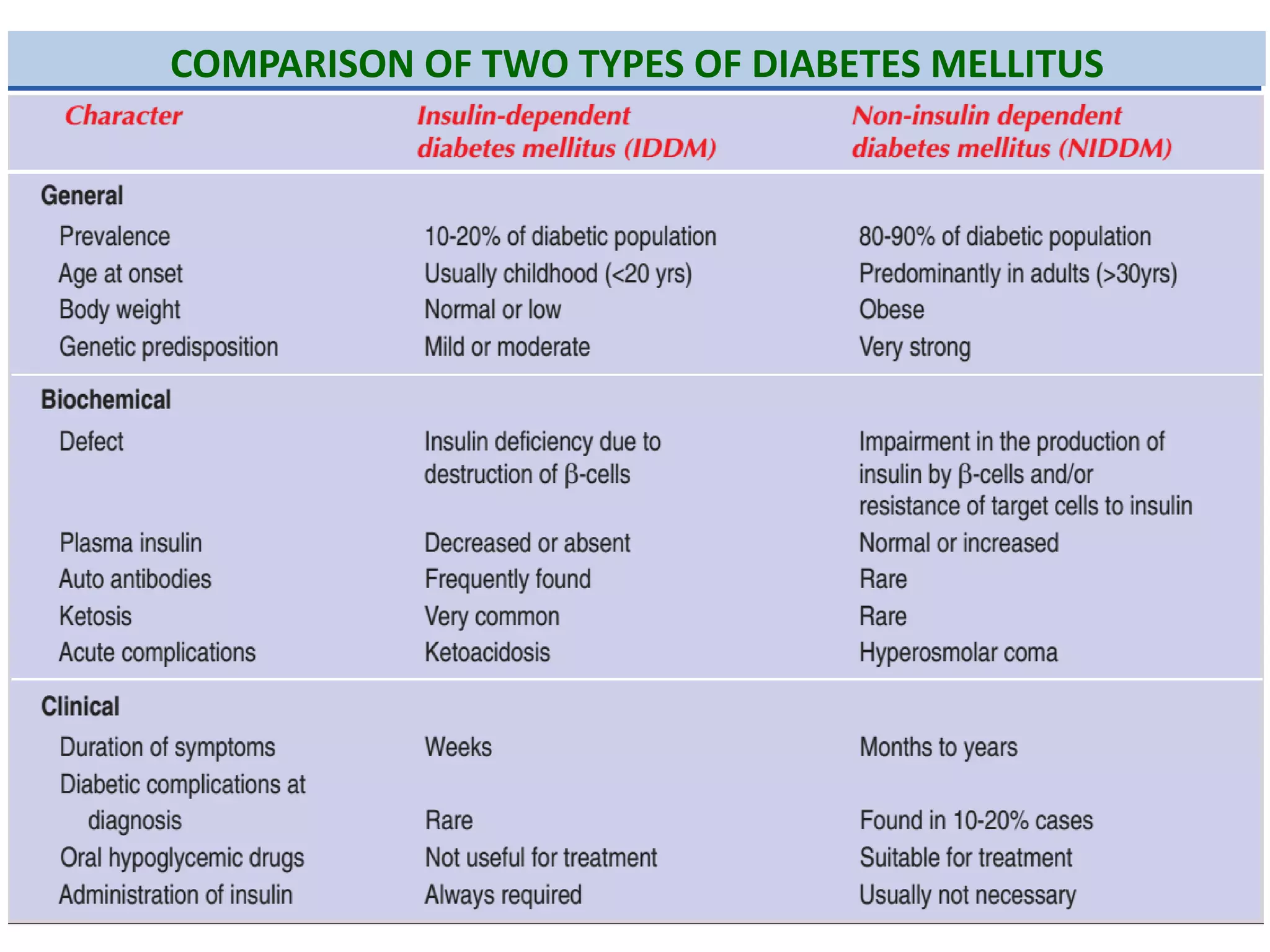
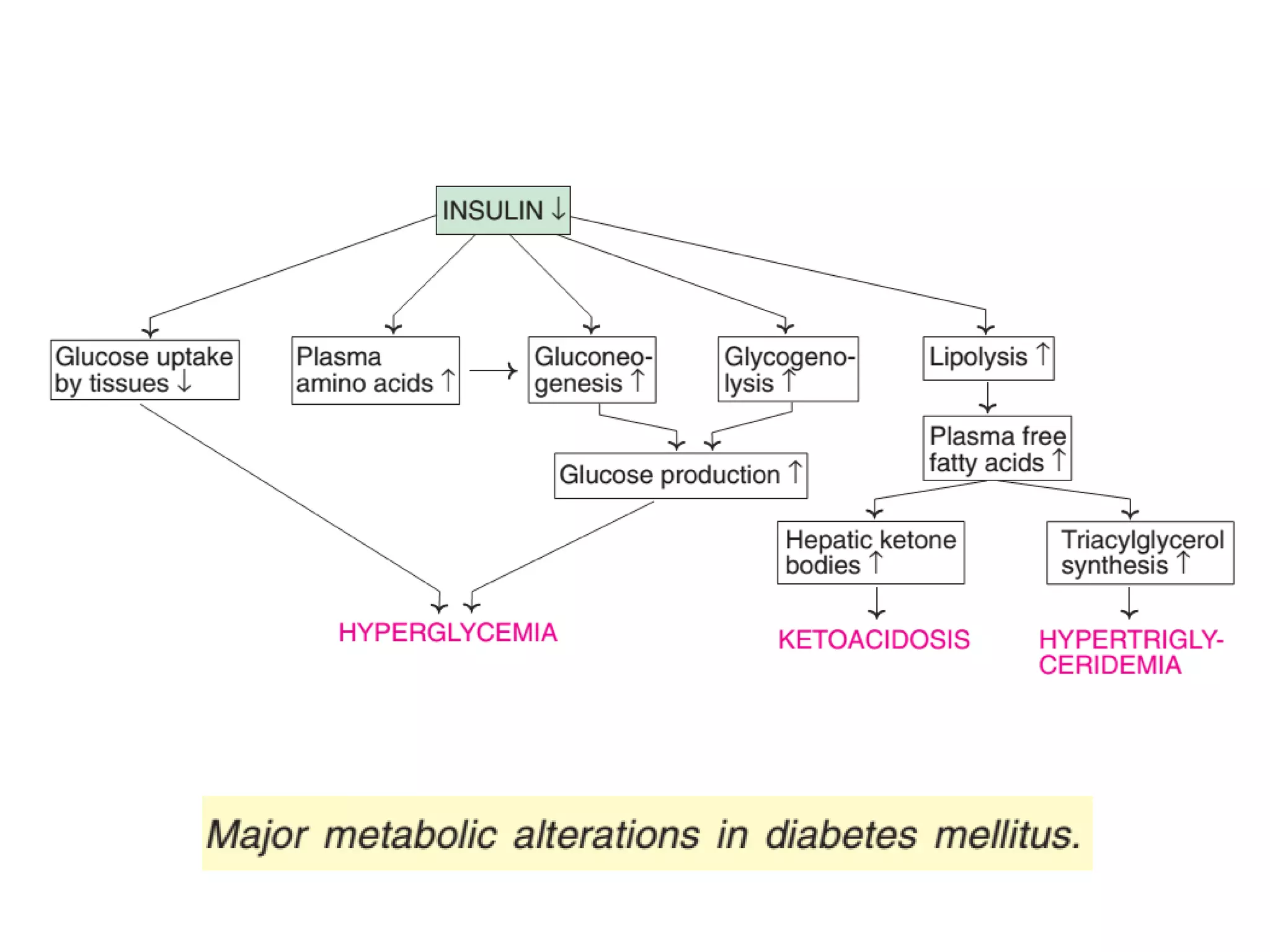
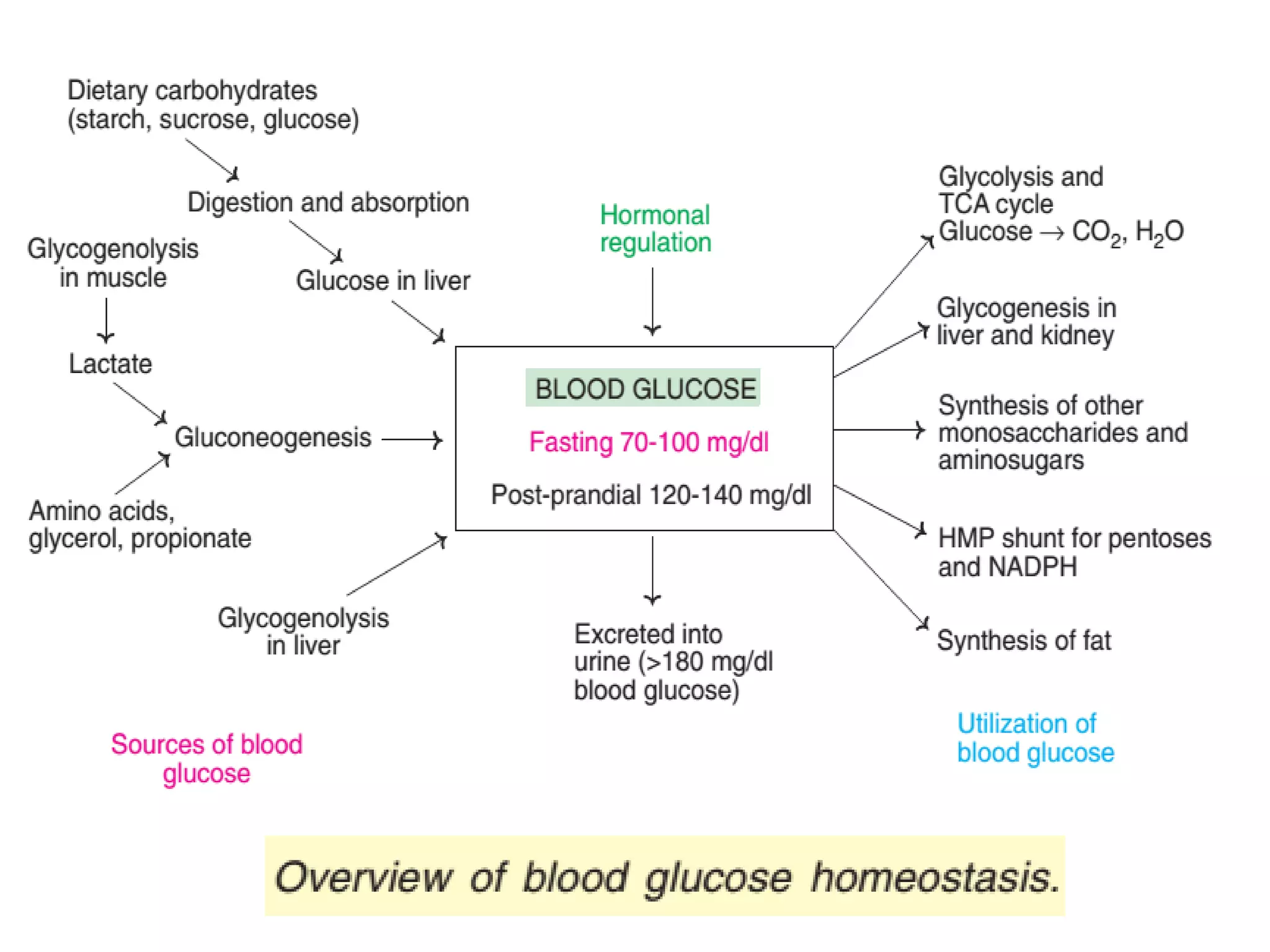
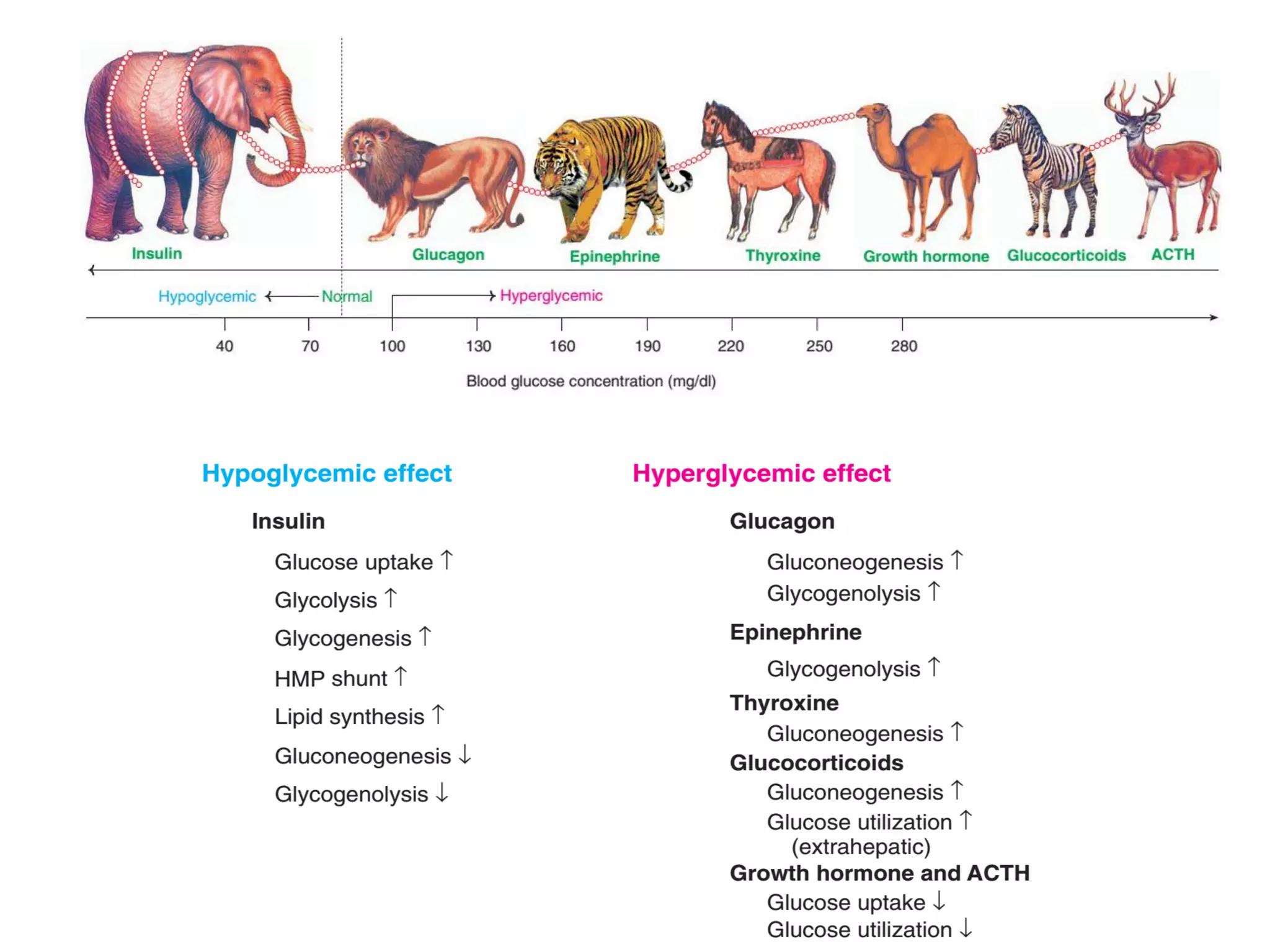
The document discusses disorders of carbohydrate and lipid metabolism. It begins by defining diabetes mellitus as a metabolic disease characterized by hyperglycemia. It then describes the two main types: insulin-dependent diabetes mellitus (IDDM), which results from destruction of insulin-producing beta cells and requires insulin treatment; and non-insulin dependent diabetes mellitus (NIDDM), which is more common and often associated with obesity. It further discusses disorders like glycogen storage diseases, pentosuria, galactosemia, and regulation of blood glucose levels. Lipid disorders like hyperlipidemia are also briefly mentioned.























































































