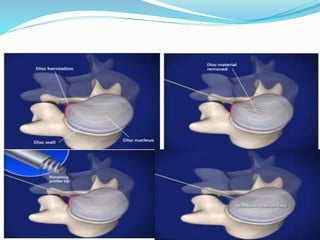
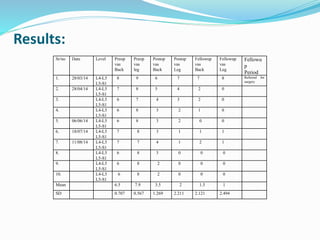
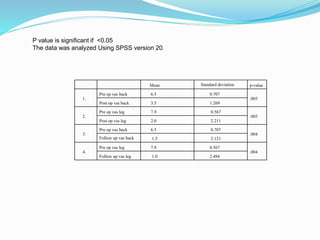
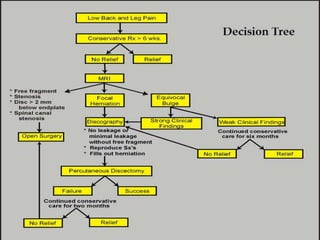
This document outlines various techniques for treating lumbar disc herniation, including chemonucleolysis and percutaneous discectomy, which are designed to alleviate related pain and improve mobility. The study details inclusion and exclusion criteria for patients, procedural methods under fluoroscopy guidance, and post-procedure care. Results indicate that these minimally invasive methods yield significant improvements in back and leg pain for selected patients.