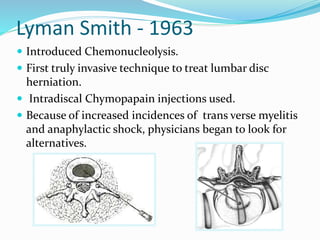
The document covers advancements in minimally invasive techniques for treating lumbar disc herniation, from early methods like chemonucleolysis to percutaneous discectomy. It outlines the criteria for patient selection, procedural techniques, and post-operative care, reporting significant improvements in pain for patients post-treatment based on collected data. The conclusion emphasizes the safety and effectiveness of these methods in skilled hands, suitable for well-selected candidates.