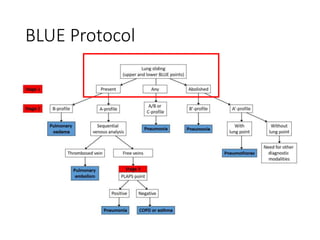
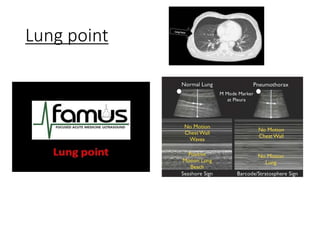
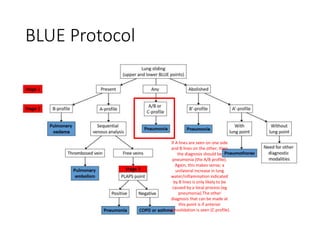
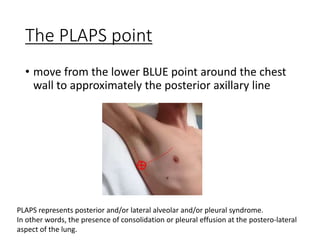
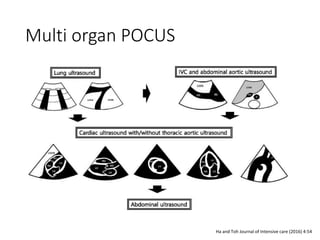
The document discusses the use of point-of-care ultrasound (POCUS) for diagnosing respiratory issues like dyspnea, chest pain, or shock, with emphasis on the Blue Protocol. It details probe selection and interpretation of ultrasound findings, including lung sliding, B lines, and A/B profiles to diagnose conditions such as pneumonia and pulmonary edema. The information aims to enhance clinical integration and effective decision-making in emergency and critical care settings.