Downloaded 25 times




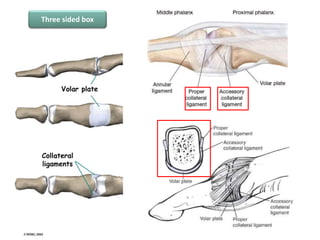

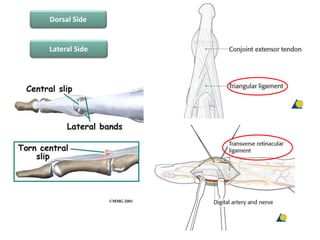

















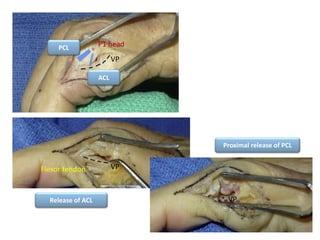
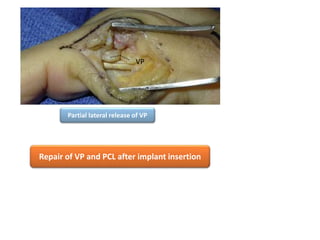

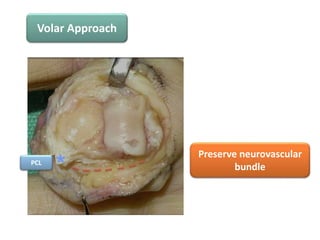



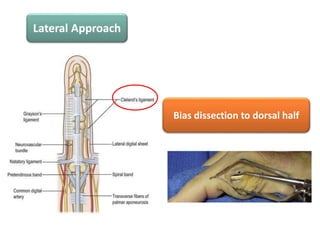









This document outlines the surgical approaches, pearls, pitfalls, and complications for proximal interphalangeal joint (PIPJ) surgery. It discusses the volar, dorsal, and lateral approaches. The volar approach is useful for implant arthroplasty, open reduction and internal fixation, and corrective osteotomies. The dorsal approach traditionally damages the extensor tendon but can be modified. The lateral approach provides access while partially releasing surrounding structures. Complications include extensor lag, poor range of motion, and disturbance to surrounding tissues. Careful surgical technique and anatomic preservation are emphasized.



































































