Downloaded 401 times































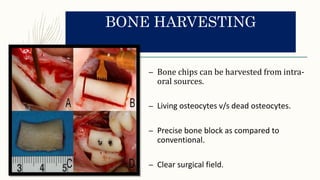
![– A total of 3,579 implants were inserted in 1,885 subjects, and the sites were prepared [with
Piezosurgery®] with a 1- to 3-year follow-up.
– No surgical complications related to the UISP protocol were reported for any of the implant
sites [and] an overall implant survival rate of 97.74% (96.99% maxilla, 98.75% mandible).](https://image.slidesharecdn.com/piezosurgery-170227135901/85/Piezosurgery-36-320.jpg)


























![– In 87.9% of the [Piezosurgery®] specimens, an outgrowth of adherent cells nearby the bone
chips was observed after 6-19 days.
– Confluence of osteoblast reached after 4 weeks.
– The morphometrical analysis revealed a statistically significant more voluminous size of the
particles collected with [Piezosurgery®] than [rotating drills].
Chiriac et al, J Clin Periodontol. 2005; 32(9):994-999](https://image.slidesharecdn.com/piezosurgery-170227135901/85/Piezosurgery-64-320.jpg)
















This document discusses piezosurgery, which uses ultrasonic vibrations from piezoelectric inserts to cut bone. Piezosurgery offers several advantages over traditional rotary cutting instruments, including more precise cuts with less risk of soft tissue or nerve damage due to lower temperatures. It allows for selective cutting of mineralized tissue without affecting elastic structures. Piezosurgery is used in various oral and maxillofacial procedures like dental implant placement, sinus lifts, orthognathic surgery, and bone harvesting. It provides better visibility, less bleeding, and more precise cuts compared to conventional techniques.



































































