Downloaded 56 times





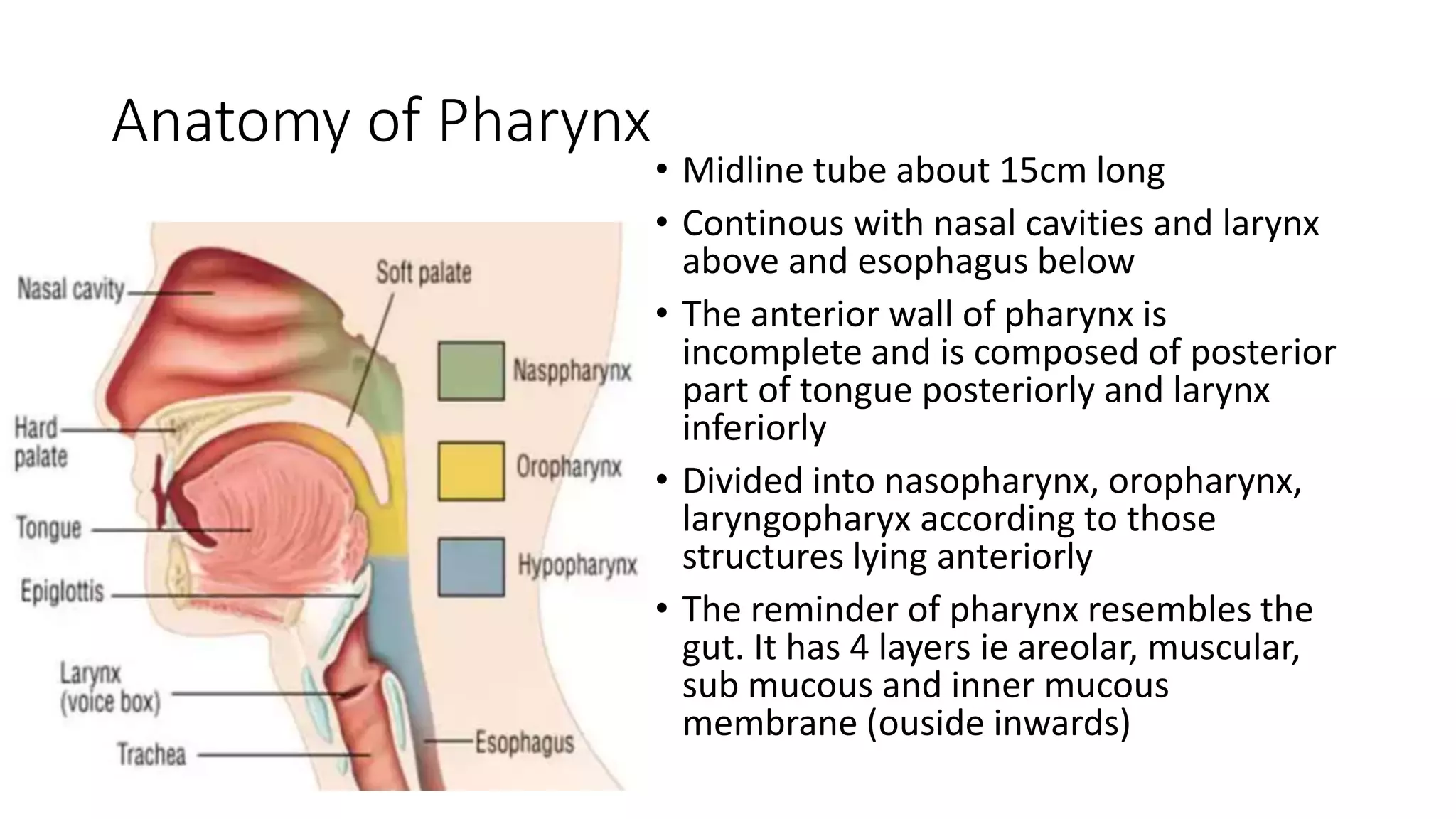



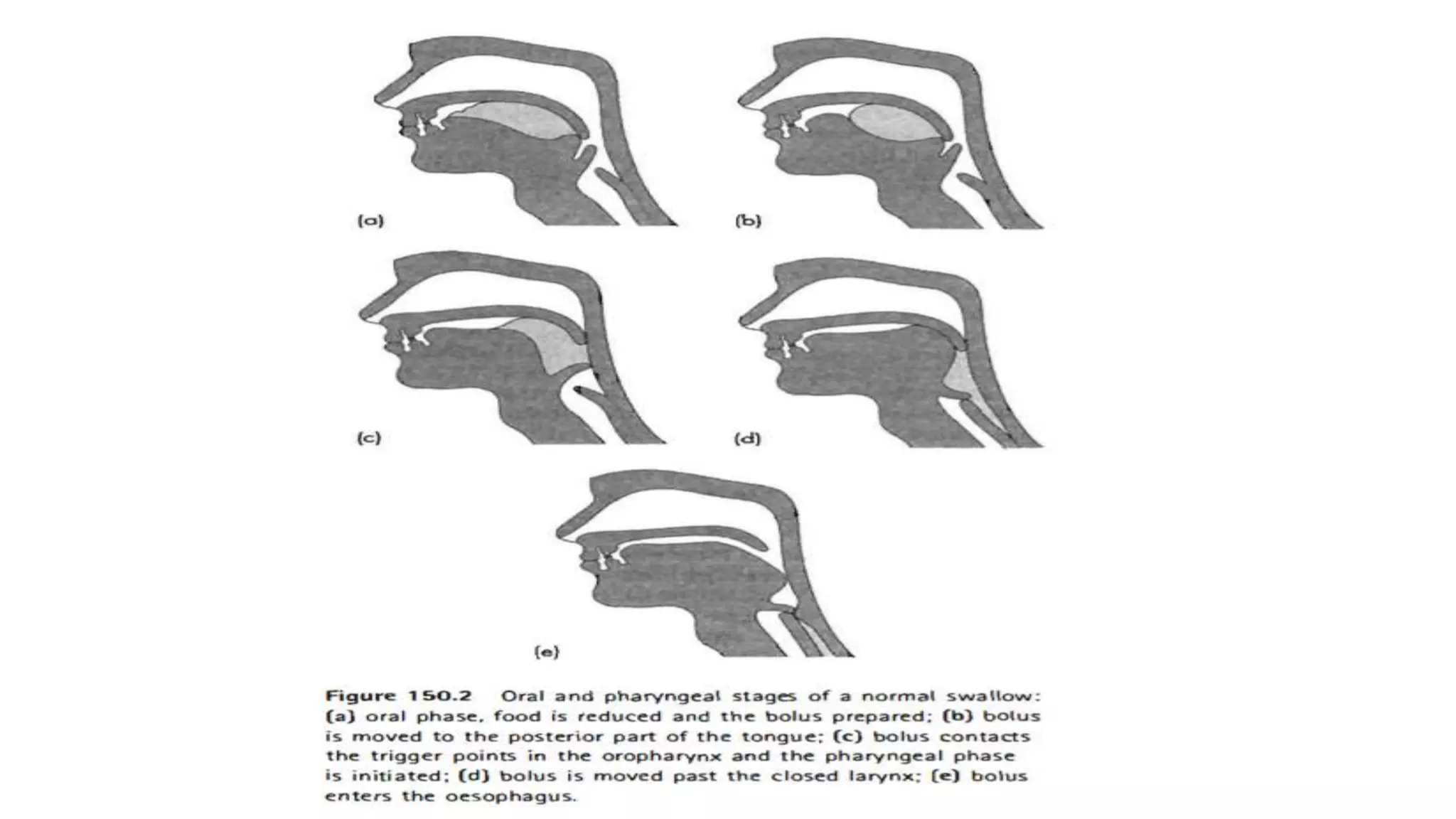




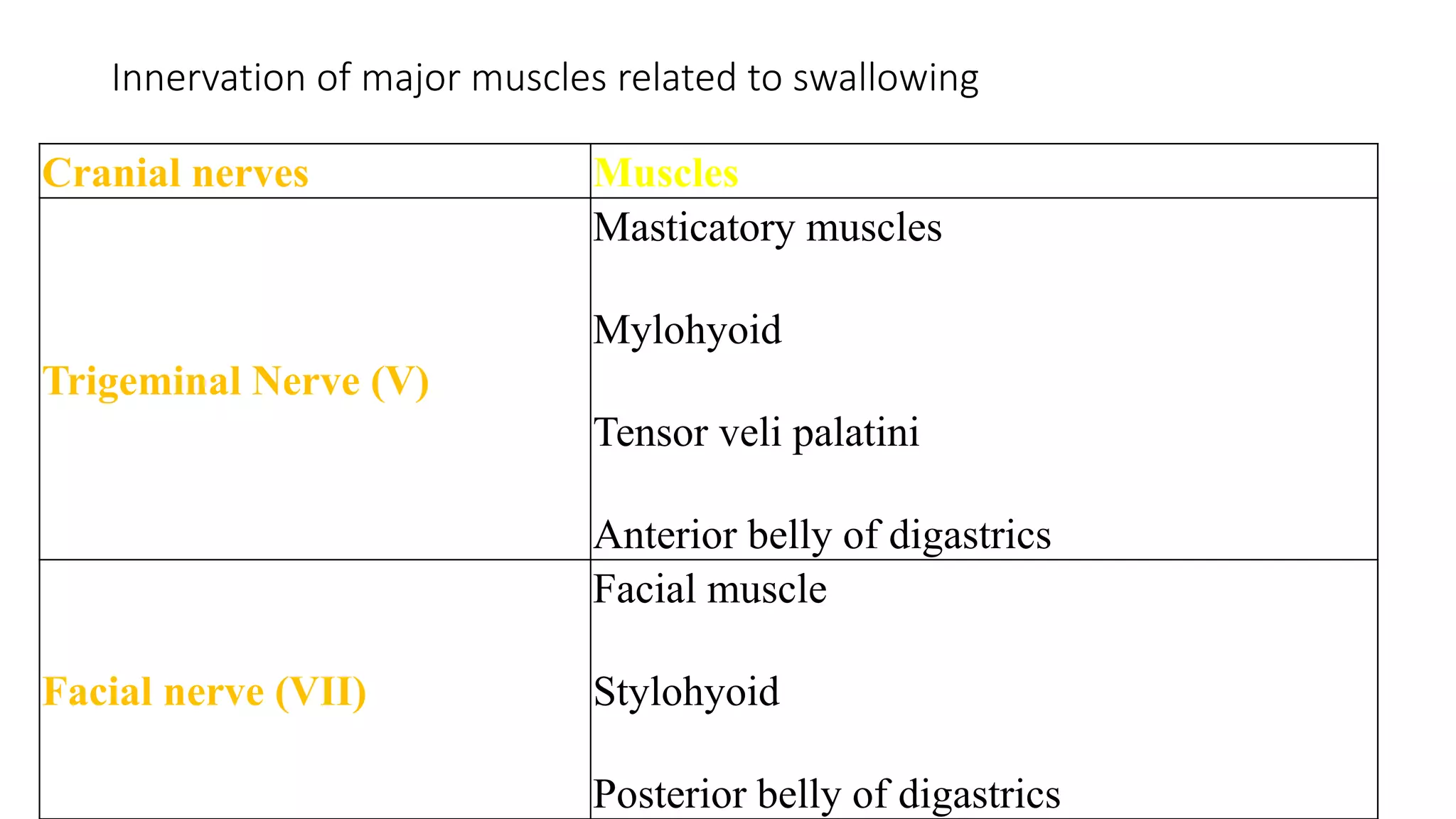














This document discusses the physiology of swallowing. It involves three phases - oral, pharyngeal, and esophageal. The oral phase involves preparing and moving food to the back of the throat using tongue and jaw muscles. The pharyngeal phase is involuntary and uses throat muscles to push food to the esophagus. The esophageal phase uses peristaltic waves to move food to the stomach through the esophagus. Swallowing is coordinated by brainstem centers and involves various cranial nerves and muscles.
































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

