Download to read offline







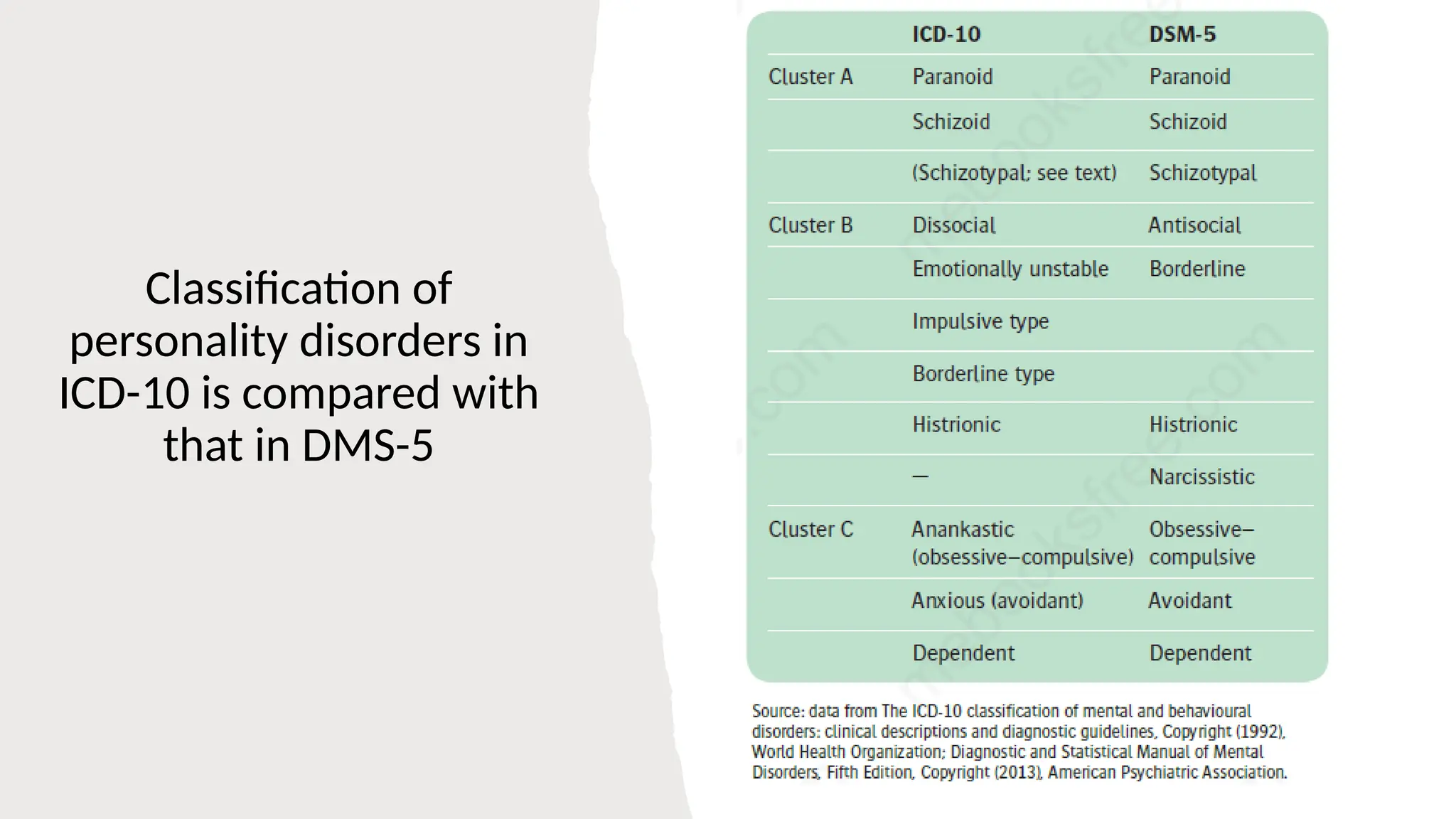




















The document provides a comprehensive overview of personality disorders, including definitions, types, prevalence, and treatment options. It categorizes personality disorders into three clusters (A, B, and C) and discusses the characteristics and implications of various disorders such as paranoid, borderline, and narcissistic personality disorders. The document emphasizes the complexity of assessing and managing these conditions due to their ingrained nature and associated comorbidities.