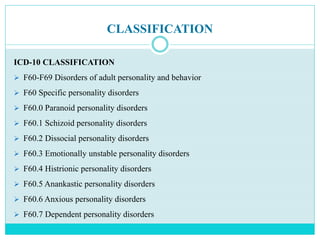

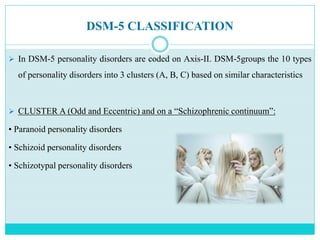
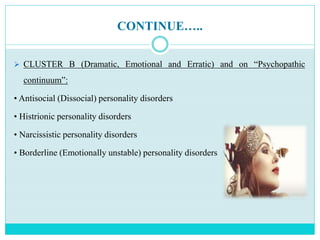
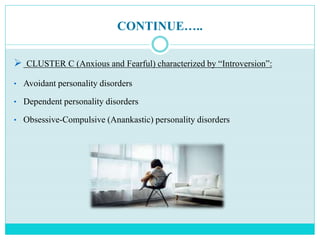
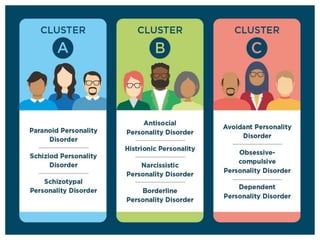
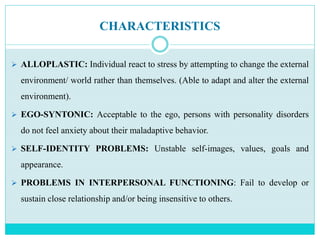
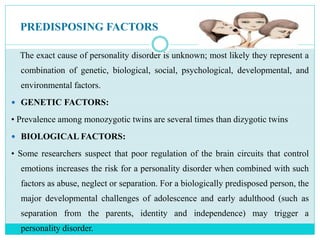
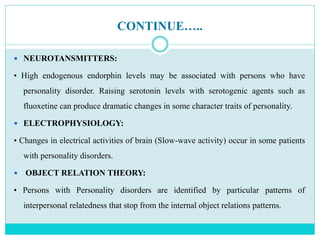



The document discusses personality disorders, examining their definitions, historical perspectives, prevalence, and classifications within ICD-10 and DSM-5 frameworks. It explains that personality disorders arise from inflexible and maladaptive traits causing social and occupational impairments and are influenced by various biological, psychological, and environmental factors. The document also highlights the core characteristics and clinical features of different personality disorders, grouped into three clusters based on similar traits, and describes their effects on individuals' emotional responses and interpersonal relationships.