Downloaded 272 times

![Papilla Preservation Flap
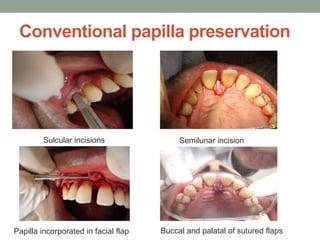
A] Conventional papilla preservation
B] Modified papilla preservation
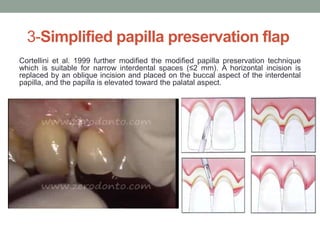
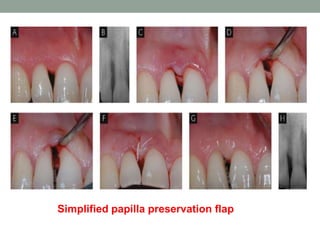
C] Simplified papilla preservation flap
D] Whale’s tail technique](https://image.slidesharecdn.com/minimalinvasivetechniques-181116162401/85/Minimal-invasive-techniques-11-320.jpg)
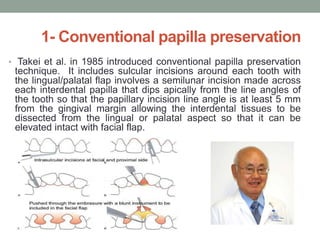



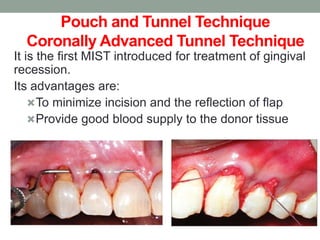





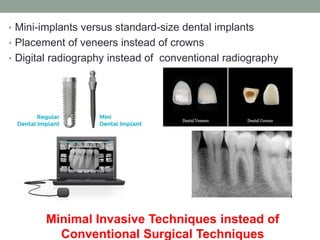
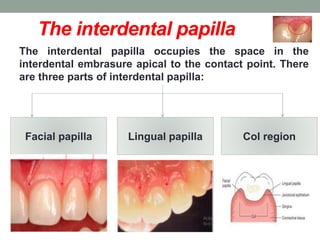
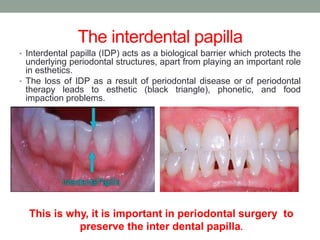
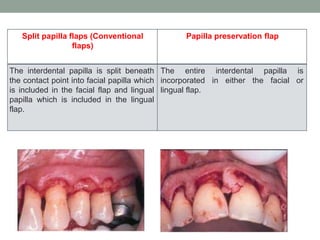
This document discusses minimal invasive techniques (MIST) in periodontal surgery. It begins by outlining some advantages of MIST such as less postoperative pain, improved healing, and better retention of soft tissues. Examples of MIST procedures described include the pouch and tunnel technique for treating gingival recession and ridge augmentation using autologous bone grafts. The document also covers papilla preservation flaps and various techniques for preserving the interdental papilla during periodontal surgery in order to maintain esthetics.