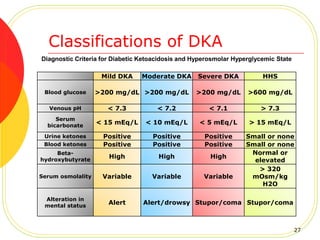
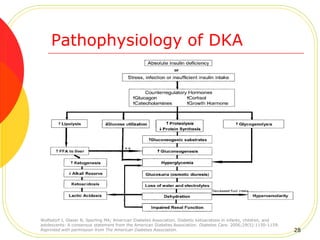
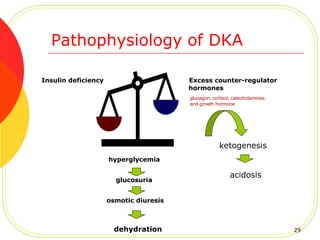
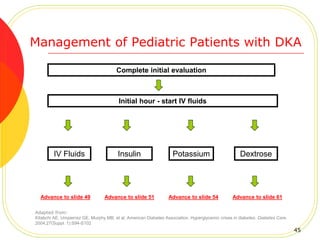
The document provides information on pediatric hyperglycemia and diabetic ketoacidosis (DKA). It defines DKA as a life-threatening condition characterized by hyperglycemia, ketosis, and acidosis. Left untreated, DKA can lead to complications and death. The document outlines the pathophysiology, clinical presentation, assessment, and management of DKA to enhance the care of pediatric patients presenting with hyperglycemia or DKA.