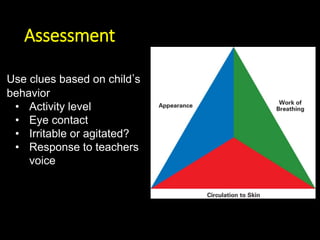
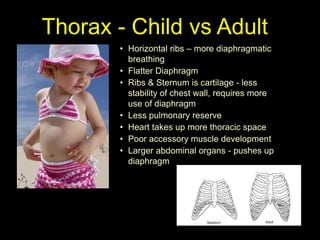
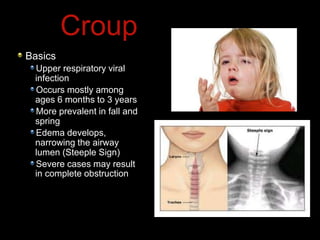
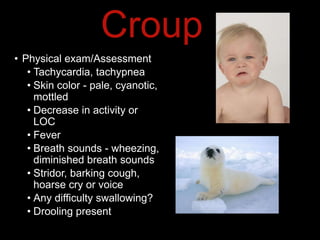
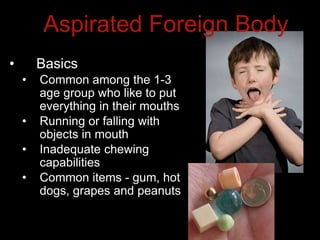
This document provides an overview of common medical emergencies that may present in school-aged children, including allergic reactions, asthma, foreign body aspiration, croup, hypoglycemia, hypovolemia, seizures, overdose/poisoning, and cardiac arrest. It reviews pediatric patient assessment, anatomical and physiological differences between children and adults, signs and symptoms, and basic life support treatment for these conditions. The objectives are to identify common pediatric emergencies, review treatment, and describe respiratory distress and failure in children.