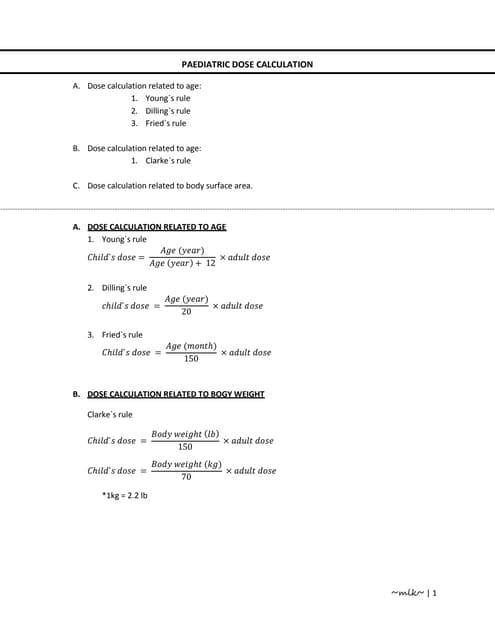
The document outlines methods for calculating and prescribing drug dosages in pediatric care, including specific dosages for commonly used drugs like aminophylline, meropenem, azithromycin, and netilmycin based on age and weight. It provides practical examples and calculations for administering medications in various scenarios, detailing infusion rates and dilution methods. The document emphasizes the importance of accuracy in dosage to ensure effective treatment in young patients.