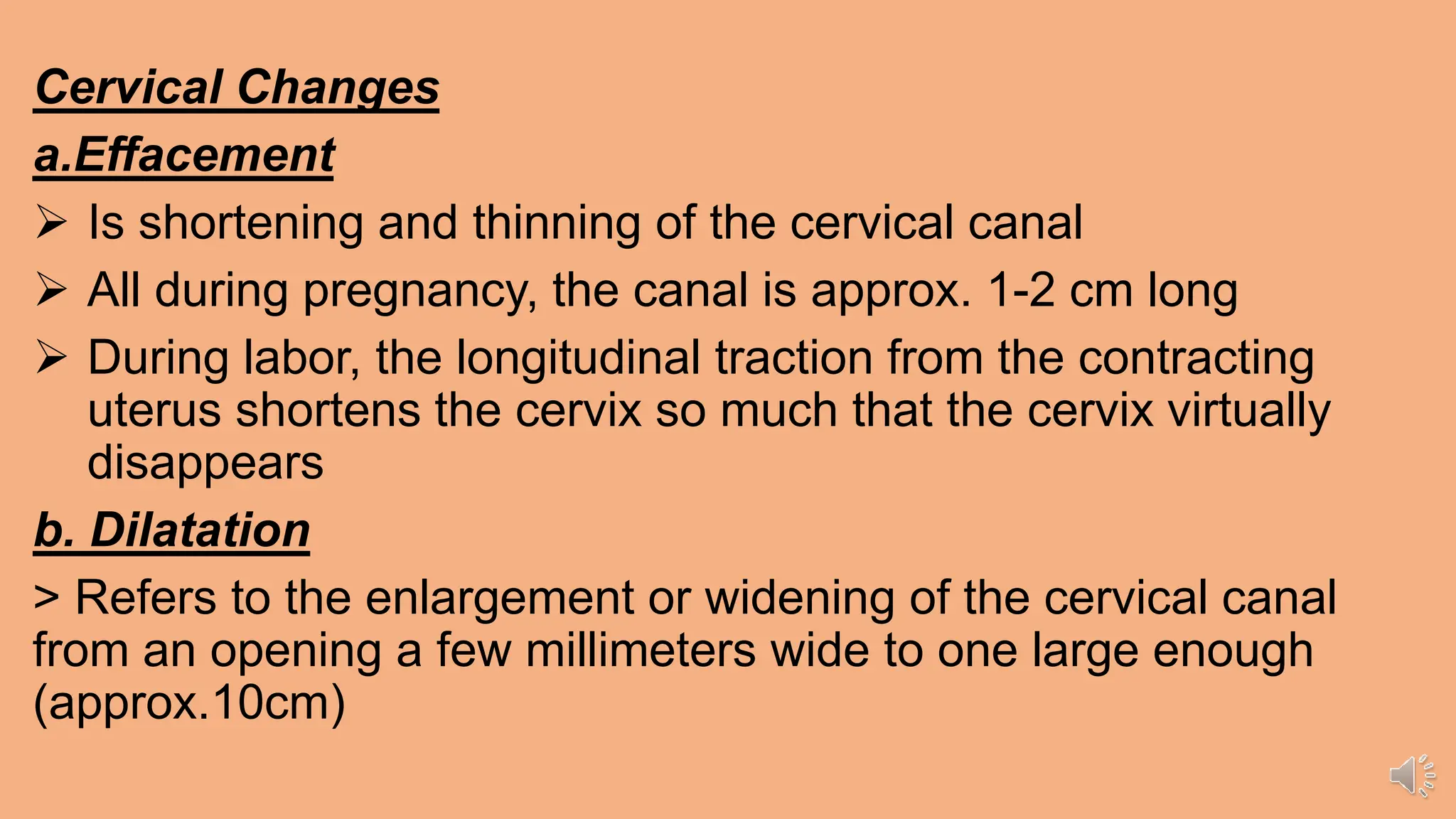
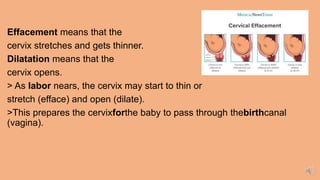
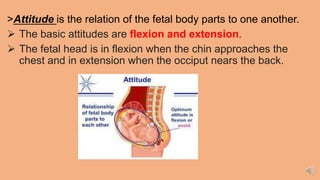
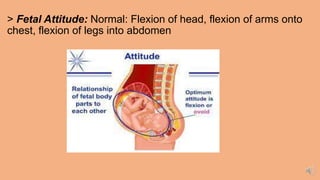
The document outlines the cervical changes during labor, including effacement and dilatation, and describes fetal attitude, lie, and presentation. It details the stages of labor, ranging from the first stage of dilatation to the third stage of placental delivery, along with nursing management and signs of maternal and fetal distress. Additionally, it discusses fetal heart rate patterns and their implications during labor.

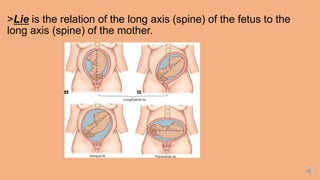
![ Position is the relation of the presenting part to the four
quadrants of the mother's pelvis.)
Position is the relationship
of the presenting part
(occiput, sacrum, mentum [chin],
or sinciput [deflexed vertex])
to the four quadrants of the
mother's pelvis](https://image.slidesharecdn.com/part2week7withrecordeddiscussion-240428122058-f5fa8d16/85/PART-2-WEEK-7-WITH-RECORDED-DISCUSSION-pptx-11-320.jpg)

































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













