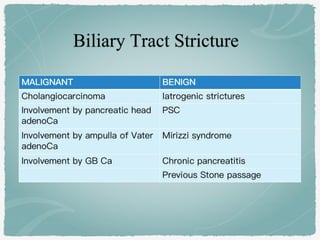
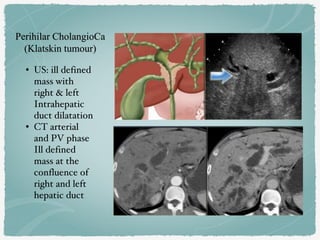
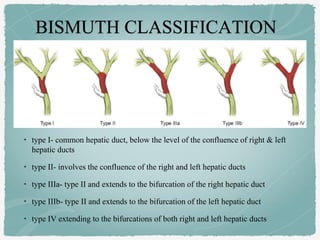
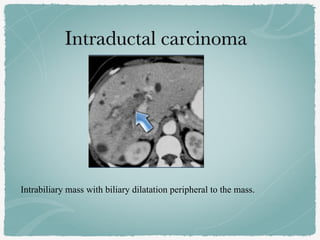
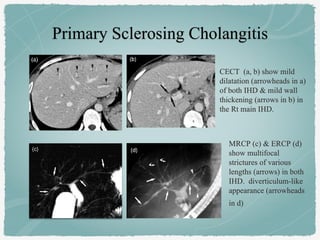
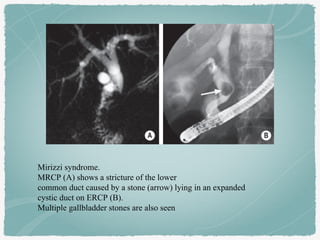
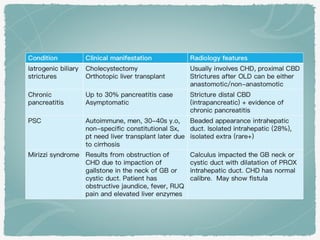
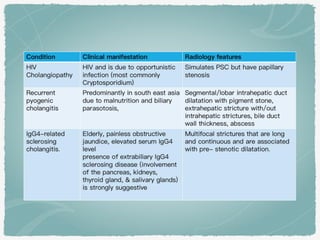
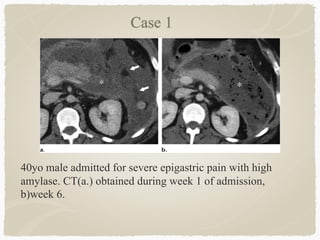
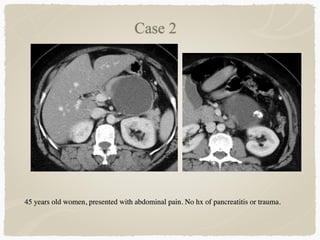
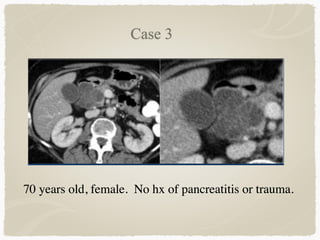
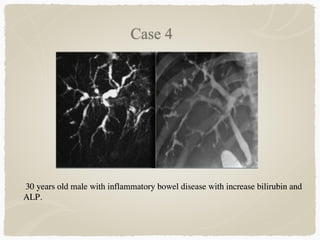
This document summarizes key information about biliary and pancreatic diseases. It discusses risk factors, epidemiology, clinical presentation, imaging features, and differential diagnosis for conditions such as cholangiocarcinoma, pancreatic cancer, autoimmune pancreatitis, and acute pancreatitis. Imaging modalities like ultrasound, CT, MRI, MRCP and ERCP play an important role in evaluation and differentiating between benign versus malignant etiologies of biliary strictures and pancreatic lesions.


























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











