This document discusses pain assessment in different populations:
- Infants feel pain from 20 weeks of gestation onward and are more sensitive to pain due to underdeveloped inhibitory neurotransmitters.
- Older adults often believe it is normal to experience pain as they age, but pain always indicates an underlying problem.
- Women generally report and display pain more than men due to biological and social factors like childbirth.
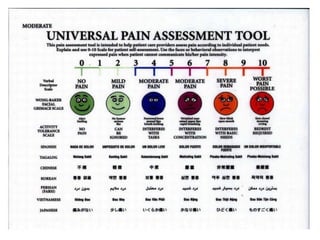
- Cultural backgrounds influence how pain is managed - for example, Hispanics tend to verbalize pain more while Asians suppress it.
- Subjective reports from patients are the most reliable indicator of pain levels. Objective measures like facial expressions are only used for non-verbal patients