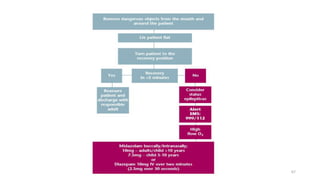
Medical Emergencies in Dental Practice discusses preparing for and managing medical emergencies that may occur during dental procedures. It outlines the responsibilities of dental practitioners to recognize emergencies and provide initial management. The document discusses common medical emergencies like syncope, hypoglycemia, angina, and their signs and symptoms. It emphasizes the importance of basic life support training for all dental office staff and having emergency equipment and medications readily available. The initial management of all medical emergencies in the dental office follows the P-C-A-B-D algorithm of positioning, circulation, airway, breathing, and definitive care.








































![MEDICAL EMERGENCIESinpd [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/medicalemergenciesautosaved-241228041041-66b7393f-thumbnail.jpg?width=640&height=640&fit=bounds)




































