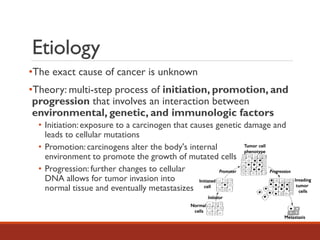
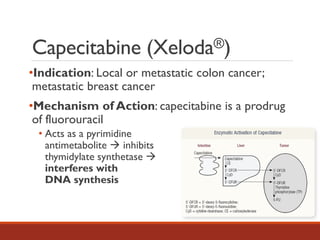
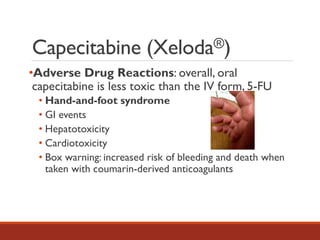
The document provides an overview of oral chemotherapy, detailing cancer epidemiology, etiology, and the pharmacology of common oral agents. It discusses specific drugs such as capecitabine, everolimus, nilotinib, and imatinib, including their indications, mechanisms of action, adverse reactions, and management. The summary emphasizes the complexity of cancer development and the clinical risks associated with both oral and parenteral chemotherapy agents.