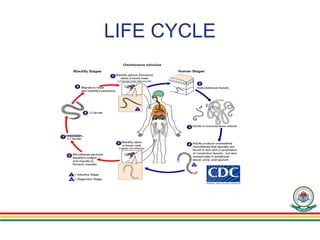
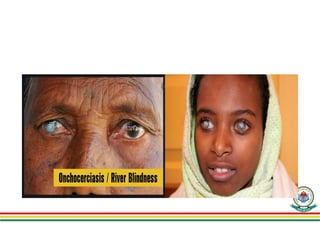
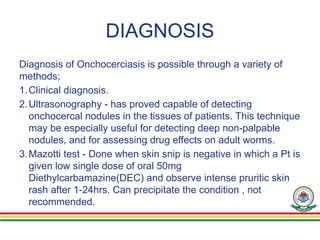
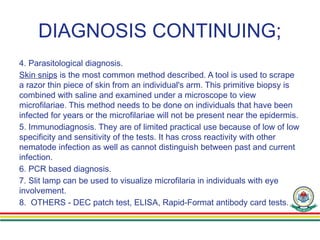
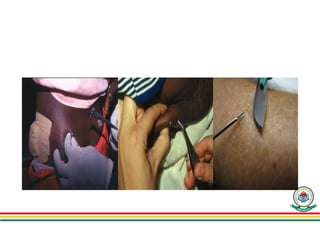
Onchocerciasis, also known as river blindness, is a filarial infection caused by the parasitic worm Onchocerca volvulus, transmitted through bites from infected blackflies. The disease primarily affects the skin and eyes, leading to severe symptoms including blindness and skin lesions, and is prevalent in 31 African countries as well as some regions in Latin America and Yemen. Diagnosis involves clinical evaluation and various tests, and treatment includes ivermectin, while vector control strategies are essential to curb transmission.


















![pp_onchocerciasis[1].pptxaaaaaaasaaaaaasaaas](https://cdn.slidesharecdn.com/ss_thumbnails/pponchocerciasis1-240912165428-6159ad61-thumbnail.jpg?width=640&height=640&fit=bounds)




























