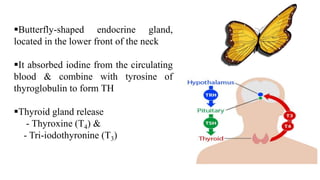
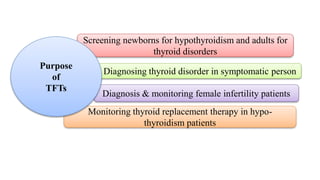
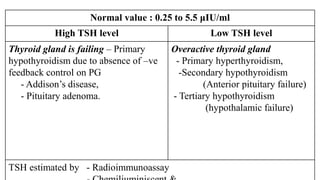
The document discusses thyroid function tests (TFTs), which measure how well the thyroid gland is working. Major TFTs include serum thyroid stimulating hormone (TSH), free thyroxine (T4) and triiodothyronine (T3), total T4 and T3, and tests for autoimmune thyroid diseases. TSH is the most sensitive and reliable test, with high levels indicating hypothyroidism and low levels indicating hyperthyroidism. Elevated or low T4 and T3 also help diagnose hypo- or hyperthyroidism. The tests help diagnose thyroid disorders, screen newborns, and monitor thyroid replacement therapy.