Downloaded 12 times

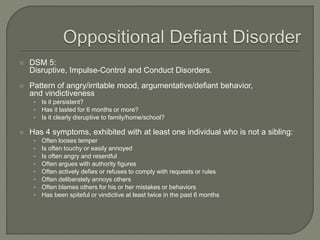
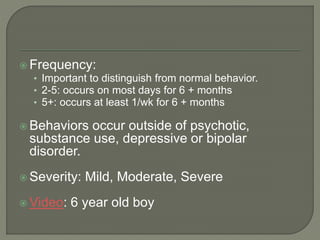





The document summarizes Oppositional Defiant Disorder (ODD), including its diagnostic criteria, prevalence rates, common behaviors, risk factors, treatment approaches, and prognosis. ODD is characterized by angry, irritable mood and argumentative/defiant behavior lasting at least 6 months. Parent-management training to improve positive parenting strategies and reduce negative ones is considered one of the most effective treatment approaches. Approximately two-thirds of children with ODD receiving treatment will be symptom-free after 3 years.











































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






