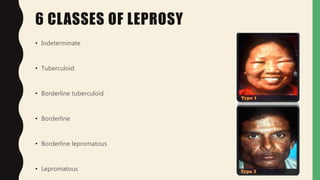
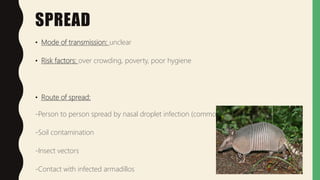
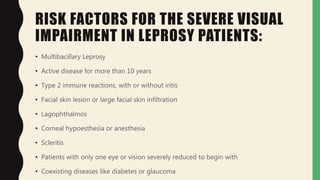
Ocular leprosy is a systemic disease caused by Mycobacterium leprae that commonly involves the eyes through hematogenous spread, resulting in uveitis. It has a prevalence of 1 in 1000 people and can cause blindness in 5-10% of ocular leprosy patients. The disease is classified into 6 types based on bacterial load and immune response. It primarily spreads through droplets from the nose but can also spread through soil, insects, or armadillos. Ocular manifestations include eyelid abnormalities, dacryocystitis, conjunctivitis, keratitis, uveitis, retinal lesions, and cranial nerve palsies. Risk factors for vision loss include multibacillary le