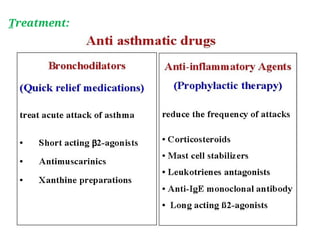
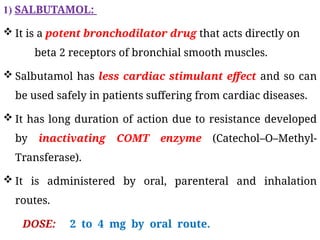
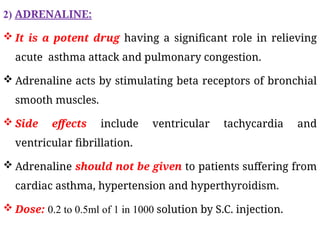
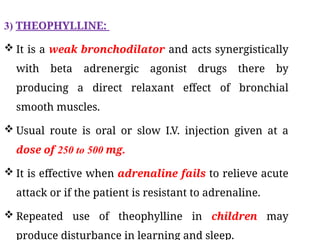
The document discusses bronchial asthma as a chronic inflammatory disorder of the airways characterized by symptoms such as breathlessness, coughing, and wheezing. It covers various aspects including epidemiology, risk factors, diagnosis, and treatment options such as bronchodilators like salbutamol and adrenaline. Complications from poorly-controlled asthma are also highlighted, emphasizing their impact on the quality of life.


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



