Downloaded 12 times

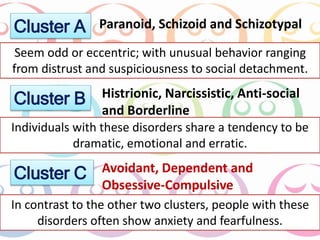













The document outlines various personality disorders, highlighting their definitions, symptoms, and treatment approaches. Specifically, it discusses paranoid and schizoid personality disorders, detailing their characteristics, prevalence, and the challenges in treatment. It emphasizes the importance of psychotherapy and the limited effectiveness of medication for these disorders, as well as the difficulties patients face in forming trusting relationships with therapists.











































































