2
Outline
◦ Physiology oflabor
◦ Mechanism of labor
◦ Diagnosis
◦ Cardinal movements of labor
◦ Normal labor characteristics
◦ Basics of parthograph reading
3.
3
Physiology of labor
◦Labor is characterized by forceful, rhythmic and painful uterine
contractions that effect cervical dilation resulting in expulsion of
products of conceptus
◦ 3 theories to describe labor initiation
◦ Functional loss of pregnancy maintenance factors
◦ Synthesis of factors that induce labor
◦ Mature fetus signaling for parturition onset
4.
4
Physiology of labor
◦Uterus
◦ Myometrium- composed of readily adaptable smooth muscle cells
surrounded by connective tissue
◦ Smooth muscle cells are in plexiform arrangement which aids the multi directional
force generation capacity of the uterus
◦ Endometrium- lines the myometrium and is transformed to decidua by
pregnancy hormones
◦ At the end of the pregnancy, the decidual activation starts
5.
5
Physiology of labor
◦Cervix has many functions
◦ Maintains a barrier to protect the reproductive tract from infection
◦ Maintains cervical competence despite gravitational forces
◦ Orchestration of extracellular matrix changes to allow for tissue compliance
◦ Placental function
◦ Exchange of nutrients and waste
◦ Source of steroid hormones, growth factors and other mediators to maintain
the pregnancy or initiate parturition
6.
6
Physiology of labor
◦Fetal membranes
◦ Amnion provides most of the membranes’ tensile strength and is
highly resistant to leukocytes and microorganisms penetration
◦ Chorion is a primarily protective tissue
◦ Sex steroid hormone
◦ Both estrogen and progesterone aid in uterine quiescence but
estrogen can also help mediate uterine activation
7.
7
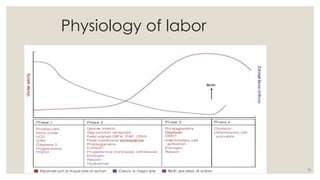
Phases of parturition
◦Partutition is arbitrarily divided into 4 overlapping phases
• Prelude to parturition
• Contractile unresponsiveness, cervical softening
Phase 1
Quiescence
• Preparation for labor
• Uterine preparedness for labor, cervical ripening
Phase 2
Activation
• Processes of labor
• Uterine contraction, cervical dilatation, fetal and
placental expulsion
Phase 3
Stimulation
• Parturient recovery
• Uterine involution, cervical repair, breast feeding
Phase 4
Involution
8.
8
Phase 1- Uterinequiescence &
cervical softening
◦ Comprises 95% of pregnancy
◦ It is characterized by uterine smooth muscle tranquility and
cervical structural integrity
◦ Uterus initiates extensive changes in its size and vascularity to
accommodate fetal growth and prepare for contractions
◦ Cervical remodeling/ softening is characterized by greater tissue
compliance but also firm and unyielding
9.
06/11/2025 9
Phase 2-Preparation for labor
◦ Progesterone withdrawal
◦ Uterine irritability and responsiveness to uterotonins by raising
oxytocin receptors
◦ Contributions from the feto-placental unit
◦ With this development, the fetal head often descends to or even
through the pelvic inlet so-called lightening
10.
10
Phase 3- Labor
◦Customarily divided into three stages
◦ The first stage begins when spaced uterine contractions bring
about cervical dilation and effacement
◦ Several uterotonins are important
◦ The second stage begins when cervical dilation is complete and
ends with delivery.
◦ The third stage is the stage of placental separation and expulsion
11.
11
Phase 4- Thepuerperium
◦ Myometrium contraction is persistent after delivery
◦ Directly compresses uterine vessels and causes thrombosis
◦ Uterotonics augment this process
◦ Remodeling involves uterine involution and cervical repair
◦ Ovulation generally occurs within 4-6 weeks
13
Mechanism of labor
Pelvicfloor changes
◦ Levator ani and fibromuscular connective tissue are the most
important components
◦ Antepartum changes in pelvic floor structure reflect adaptation
which permits vaginal delivery
◦ During pregnancy, levator ani hypertrophies but with labor,
stretching of the muscle results in thinning of the perineum
14.
14
Mechanism of labor
Fetallie
◦ Relationship of the fetal long axis to that of the mother
◦ Longitudinal [99%], transverse, oblique
Presentation
◦ The presenting part is the part of fetal body that is within the birth
canal
◦ According to fetal lies, presentations can be
◦ Longitudinal- cephalic & breech
◦ Transverse- shoulder
Longitudinal lie
Oblique lie
Transverse lie
15.
15
Mechanism of labor
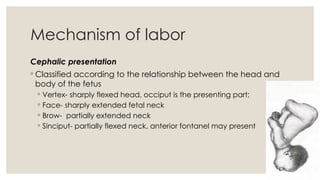
Cephalicpresentation
◦ Classified according to the relationship between the head and
body of the fetus
◦ Vertex- sharply flexed head, occiput is the presenting part;
◦ Face- sharply extended fetal neck
◦ Brow- partially extended neck
◦ Sinciput- partially flexed neck, anterior fontanel may present
16.
16
Mechanism of labor
Attitude
◦It is the position of the fetal head and neck to the fetal body
Position
◦ The relationship of the fetal presenting part to the right or left side of the
pelvis or anterior, transverse or posterior position to the maternal pelvis
◦ Based on the presenting part
◦ Occiput - Vertex presentation
◦ Mentum - Face presentation
◦ Sacrum - Breech presentation
18
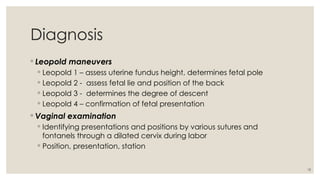
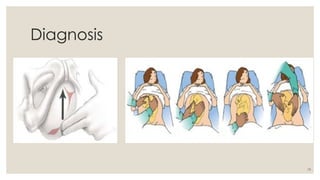
Diagnosis
◦ Leopold maneuvers
◦Leopold 1 – assess uterine fundus height, determines fetal pole
◦ Leopold 2 - assess fetal lie and position of the back
◦ Leopold 3 - determines the degree of descent
◦ Leopold 4 – confirmation of fetal presentation
◦ Vaginal examination
◦ Identifying presentations and positions by various sutures and
fontanels through a dilated cervix during labor
◦ Position, presentation, station
21
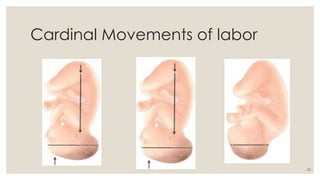
Cardinal movements oflabor
ENGAGEMENT
◦ Mechanism where BPD passes through the pelvic inlet
◦ Occurs before labor in nulliparous and after onset of labor in
multiparous
◦ Commonly with OT position
DESCENT
◦ Brought about by
◦ Direct pressure of the fundus on breech with contractions
◦ Maternal bearing down efforts
◦ Extension and straightening the fetus
22.
22
Cardinal movements oflabor
FLEXION
◦ Occurs when descending head meets resistance- from the cervix
or pelvic floor
◦ It brings the chin closer to the thorax and the shorter suboccipito
bregmatic diameter presents
INTERNAL ROTATION
◦ It turns occiput away from the transverse axis
◦ It is essential for completion of labor
06/11/2025 24
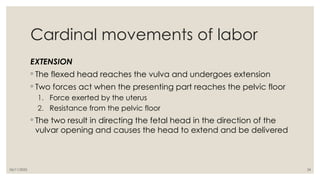
Cardinal movementsof labor
EXTENSION
◦ The flexed head reaches the vulva and undergoes extension
◦ Two forces act when the presenting part reaches the pelvic floor
1. Force exerted by the uterus
2. Resistance from the pelvic floor
◦ The two result in directing the fetal head in the direction of the
vulvar opening and causes the head to extend and be delivered
25.
25
Cardinal movements oflabor
EXTERNAL ROTATION
◦ The delivered head undergoes restitution
◦ After completion of the restitution, the head rotates to a
transverse position- placing the anterior shoulder under the
symphysis pubis
EXPULSION
◦ Commonly the anterior shoulder is delivered first, followed by the
posterior
◦ The rest of the body passes
26.
26
Cardinal movements oflabor
FETAL HEAD SHAPE CHANGES
◦ Labor forces alter fetal head shape
◦ Caput succedaneum - the swelling on the part of the fetal scalp
over the cervical os
◦ Molding - changes in the fetal bony head due to external
compressive forces
◦ It results in a shortened suboccipito-bregmatic diameter
27.
27
Normal labor characteristics
◦Diagnosis of labor is retrospective
FIRST STAGE OF LABOR
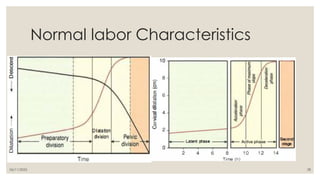
◦ Friedman developed the concept of 3 functional labor divisions
◦ Preparatory division
◦ Dilatational division
◦ Pelvic division
29
Normal labor characteristics
Latentphase
◦ Starts with onset of regular contractions
◦ Up to 4-5 cm
◦ It can extend up to 20 hours in nulliparous women and 14 hours in
multiparous women
30.
30
Normal labor characteristics
Activephase
◦ Represented by cervical dilation of 6cm or more in the presence
of uterine contractions
◦ Rate of cervical dilation
◦ Nulliparous – 1.2cm/hour
◦ Multiparous – 1.5cm/hour
◦ Descent begins in the later stages of active phase
31.
31
Normal labor characteristics
SECONDSTAGE
◦ Starts with complete cervical dilation and ends with fetal delivery
◦ Median duration
◦ Nulliparous - 50 minutes
◦ Multiparous – 20 minutes
32.
32
Normal labor characteristics
Managementof normal labor
1. Recognize normal physiological process of labor
1. Initial evaluation – history, physical exam – cervical assessment
2. Anticipate intrapartum complications
1. Intrapartum fetal monitoring
2. Maternal monitoring
3. Make every woman feel supported and comfortable
1. Oral intake
2. Maternal positioning
34
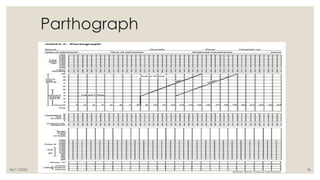
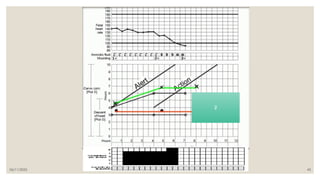
Parthograph
◦ It isa graphic representation of the progress of labor
◦ It is started during active phase of labor
◦ Advantages
◦ Detects abnormal labor
◦ It aids in recognizing cephalopelvic disproportion before obstruction
occurs
◦ It serves as an early warning system and important for timing of
decision
35.
35
What is plottedon parthograph?
◦ Identification
◦ Progress of labor
◦ Cervical dilatation
◦ Descent of fetal head
◦ Uterine contractions
◦ Fetal condition
◦ Fetal heart rate
◦ Membranes status and liquor
◦ Moulding of fetal skull
◦ Maternal condition
◦ Pulse/BP/Temp
◦ Urine – volume, protein
◦ Medications and IV fluids
◦ Oxytocin
06/11/2025 37
Parthograph
◦ Cervicaldilatation is plotted with an ‘X’
◦ Pelvic exams are done every 4 hours with some exceptions
◦ Descent is measured based on the fetal head above the pelvic brim in
terms of fingers(5)
◦ Descent is marked by ‘O’
◦ Expressed interms of 0-5
38.
06/11/2025 38
Parthograph
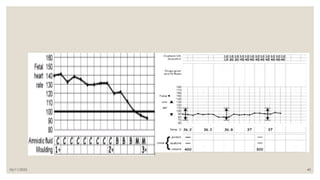
◦ Uterinecontractions are monitored and plotted every 30 minutes,
duration and frequency over 10 minutes
◦ Fetal heart rate
◦ Counted for one minute after a contraction passes
◦ Membrane status and liquor are recoded
◦ Intact- I
◦ Clear – C
◦ Meconium – M
◦ Absent –A
◦ Blood stained - B
39.
39
Parthograph
◦ Fetal conditionlike molding are also reported
◦ Molding
◦ Bones are separated and sutures felt
◦ Bones are just touching each other
◦ Bones are overlapping
◦ Bones are overlapping severely
◦ Maternal condition
◦ Pulse- every 30 minutes
◦ BP & temperature – every 4 hours
06/11/2025 41
Abnormal Parthograph
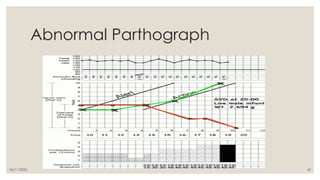
◦In active phase, cervical dilatation will remain on the left of or on
the alert line
◦ Action line is 4 hours to the right of the alert line
◦ Once action line is crossed, action should be taken
#3 Labor is the last hours of pregnancy
Extensive preparations take place in both the uterus and cervix
During the first 36 to 38 weeks of normal gestation, the myometrium is in a preparatory yet unresponsive state.
Following this prolonged uterine quiescence, a transitional phase follows during which myometrial unresponsiveness is suspended and the cervix undergoes ripening, effacement, and loss of structural cohesion.
Current research supports a model that draws from all three themes
#4 the smooth muscle cell is not terminally differentiated and therefore is readily adaptable to environmental changes such as mechanical stretch, inflammation, and endocrine and paracrine signals
Composed of stromal cells and maternal immune cells, the decidua maintains the pregnancy by suppressing inflammatory signals during gestation. [promotes an environment of immune tolerance to protect the fetus. Namely, decidual stromal cells proactively ensure that fetal antigens do not elicit a maternal immune response. his stems from a reduced capacity to attract T cells.]
Decidual activation- the decidua transitions to induce inflammatory signals and withdraw active immunosuppression, which contribute to parturition initiation
#5 In nonpregnant women, the cervix is closed and firm,
and its consistency is similar to nasal cartilage. By the end of
pregnancy, the cervix is easily distensible, and its consistency
is similar to the lips
#6 The fetal membranes-amnion and chorion and adjacent decidua-make up an important tissue shell around the fetus that serves as a physiological, immunological, and metabolic shield to protect against untimely parturition initiation
Chorion - It is also enriched with enzymes that inactivate uterotonins, which are agents that stimulate contractions.
Progesterone withdrawal, directly precedes progression of parturition
#7 parturition can be arbitrarily divided into four overlapping phases that correspond to the major physiological transitions of the myometrium and cervix during pregnancy
Importantly, the phases of parturition should not be confused with the clinical stages of labor, that is, the first, second, and third stages-which make up phase 3 of parturition
#8 some low-intensity myometrial contractions are felt during the quiescent phase, but they do not normally cause cervical dilation. referred to as Braxton Hicks contractions or false labor
To ensure uterine quiescence, the synthesis in the decidua of prostaglandins is markedly suppressed
Key to matrix changes, collagen undergoes conformational changes that alter tissue stiffness and flexibility
#9 CRH hormone that is identical to maternal and fetal hypothalamic CRH is synthesized by the placenta in relatively large amounts
However, unlike hypothalamic CRH , which is under glucocorticoid negative feedback, cortisol instead stimulates placental CRH production. In the last 12 weeks, CRH plasma levels rise exponentially, peak during labor
Fetal contributions- uterine stretch increases oxytocin receptors, fetal endocrine cascades
#10 The upper segment is firm during contractions, whereas the lower
segment is softer, distended, and more passive
Mechanical stretching of the cervix enhances uterine activity-Ferguson reflex
If the lower uterine segment and cervix, were to contract simultaneously and with equal intensity, the net expulsive force would markedly decline. Thus, the upper segment contracts, retracts, and expels the fetus. In response to these contractions, the softened lower uterine segment and cervix dilate and thereby form a greatly expanded, thinned-out tube through which the fetus can pass
he myometrium of the upper segment does not relax to its
original length after contractions. As the consequence of retraction,
each successive contraction commences where its predecessor
left off.
in the lower segment, successive lengthening of the
fibers with labor is accompanied by thinning is a result of the lower
segment thinning and concomitant upper segment thickening,
a boundary between the two is marked by a ridge on the inner
uterine surface-the physiological retraction ring
ANCILLARY forces- the most important force in fetal expulsion is produced by maternal intraabdominal pressure
Contraction of the abdominal muscles simultaneously with
forced respiratory efforts with the glottis closed is referred to
as pushing
CERVICAL effacement -shortening of the cervical canal from a length of approximately 3 cm to a mere circular orifice with almost paper-thin edges.
As uterine contractions cause pressure on the membranes, the hydrostatic action of the amniotic sac in turn dilates the cervical canal. With ROM the presenting fetal part is positioned to exert pressure against the cervix and lower segment.
cervical dilation is divided into latent and active phases. The active phase is subdivided further into the acceleration phase, the phase of maximum slope, and the deceleration phase.
Second stage- speed of descent is maximal and is maintained until the presenting part reaches the perineal floor
PELVIC FLOOR CHANGES
#11 Remodeling- returns these organs to the non pregnant state
-protect from MO invasion and restore responsiveness to normal hormones
#13 The levator ani muscle varies in thickness from 3 to 5 mm,
although its margins encircling the rectum and vagina are somewhat thicker. This is accompanied by thinning of the central portion
of the perineum, which becomes transformed from a wedgeshaped, 5-cm-thick tissue mass to a thin, almost transparent
membranous structure less than 1 cm thick
#14 transverse lie is less frequent,and predisposing factors include multiparity, placenta previa,hydramnios, and uterine anomalies
the fetal and maternal axes may cross at a 45-degree angle, forming an oblique lie. his is unstable and becomes longitudinal or transverse during labor.
#15 The term fetus usually presents with the vertex, most logically because the uterus is pear shaped. The fetus orients its polarity to make use of the roomier fundus for its bulkier and more mobile podalic pole.
Ordinarily, the head is flexed sharply so that the chin contacts the thorax.
Much less often, the fetal neck may be sharply extended so that the occiput and back come into contact latter
Two are usually transient.
As a rule, the fetus forms an ovoid mass that corresponds roughly to the shape of the uterine cavity. The fetus becomes folded upon itself to create a convex back. The head is sharply flexed; the chin is almost in contact with the chest; the thighs are flexed over the abdomen; and the legs are bent at the knees.
#16 Approximately two thirds of all vertex presentations are in the left occiput position, and one third in the right
#18 Several methods can be used to diagnose fetal presentation and position. Abdominal examination can be conducted systematically
employing the four maneuvers described by Leopold in 1894
mother lies supine and comfortably positioned with her abdomen bared
The breech gives the sensation of a large, nodular mass, whereas the head feels hard and round and is more mobile.
The second maneuver is accomplished as the palms are placed on either side of the maternal abdomen, and gentle but deep pressure is exerted. On one side, a hard, resistant structure is felt-the back. On the other, numerous small, irregular, mobile parts are felt-the fetal extremities
3rd thumb and fingers of one hand grasp the lower portion of the maternal abdomen j just above the symphysis pubis. If the
presenting part is not engaged, a movable mass will be felt, usually the head.
4th- examiner faces the mother's feet, and the fingertips of both hands are positioned on either side of the presenting
part. They exert inward pressure and then slide caudad along the axis of the pelvic inlet.
Leopold maneuvers with a high sensitivity-88 percent, speciicity-94 percent, positive- predictive value-74 percent, and negative-predictivevalue-97 percent
Vaginal exam- if vertex is presenting , insert fingers posteriorly then sweep anteriorly where sagittal suture is crossed. and its linear course is delineated. Next, the positions of the two fontanels, found at either end of the sagittal suture, are ascertained
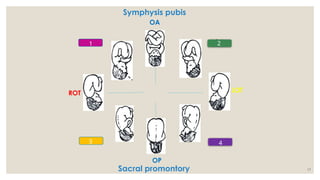
#20 The positional changes of the presenting part required to
navigate the pelvic canal constitute the mechanisms of labor
In most cases, the vertex enters the pelvis with the sagittal suture
lying in the transverse pelvic diameter. The fetus enters the pelvis
in the (LOT) position more commonly than (ROT) position
During labor, these movements not only are sequential but also show great temporal overlap-example, as part of engagement, there is both flexion and descent of the head
Descent
#21 Concomitantly, uterine contractions effect important modifications in fetal attitude
BPD- greatest transverse diameter in an occiput presentation
The sagittal suture frequently is deflected either posteriorly toward the promontory or anteriorly toward the symphysis
lateral deflection to a more anterior or posterior position in the pelvis is called asynclitism.
If the sagittal suture approaches the sacral promontory, more of the anterior parietal bone presents itself, anterior asynclitism
Moderate degrees of asynclitism are the rule in normal labor
Descent -This movement is the first requisite for birth.
#22 With this movement, the chin is brought into more intimate contact with the fetal thorax, and the appreciably shorter suboccipitobregmatic diameter is substituted for the longer occipitofrontal diameter
IR-Usually the occiput rotates anteriorly toward the symphysis pubis, but less commonly, it may rotate posteriorly
internal rotation is completed by the time the head reaches the pelvic floor
#24 If the sharply flexed head, on reaching the pelvic floor, did not extend but was driven farther downward, it would impinge on the posterior portion of the perineum and would eventually be forced through the perineal tissues
The first force, exerted by the uterus, acts more posteriorly, and the second, supplied by the resistant pelvic floor and the symphysis, acts more anteriorly
#25 Restitution- If the occiput was originally directed toward the left/right, it rotates toward the left/right ischial tuberosity
Restitution - This movement corresponds to rotation of the fetal body and serves to bring its bisacromial diameter into relation with the anteroposterior diameter of the pelvic outlet.
#26 It usually attains a thickness of only a few millimeters, but in prolonged labors it may be sufficiently extensive to prevent differentiation of the various sutures and fontanels.
Most studies indicate that there is seldom overlapping of the parietal bones. A "locking" mechanism at the coronal and lambdoidal sutures actually prevents such overlapping
The degree to which the head is capable moldling may make the diference between spontaneous vaginal delivery and an operative
delivery.
#27 during the preparatory division, although the cervix dilates little, its connective tissue components change considerably
dilational division, during which dilation proceeds at its most rapid rate
Pelvic division commences with the deceleration phase of cervical dilation.
Two phases of cervical dilation are defined.
The latent phase corresponds to the preparatory division, and the active phase to the dilational division
Friedman further subdivided the active phase into the acceleration phase, the phase of maximum slope, and the deceleration phase (
#30 Descent begins in the later stage of active dilation, commencing at 7 to 8 cm in nulliparas and becoming most rapid after 8 cm.
Active phase disorders- protraction and arrest
#37 When progress of labor is normal, plotting of cervical dilatation remains on the alert line or to the left of it
the head is engaged when the portion of the head above the brim is represented by 2 fingers are less
Descent is plotted with an “O’ on the Partograph
#38 Counted for a full minute
Every 30 minutes
FHR- if abnormal over 3 observations- take action
#41 At or beyond action line- delivery if fetal distress or CPD
Oxytocin augmentation if no c/I
Supportive therapy
![14
Mechanism of labor
Fetal lie
◦ Relationship of the fetal long axis to that of the mother
◦ Longitudinal [99%], transverse, oblique
Presentation
◦ The presenting part is the part of fetal body that is within the birth
canal
◦ According to fetal lies, presentations can be
◦ Longitudinal- cephalic & breech
◦ Transverse- shoulder
Longitudinal lie
Oblique lie
Transverse lie](https://image.slidesharecdn.com/presentationnormallabor-250611133016-fd4db04a/85/Presentation-Normal-labor-ppsx-in-health-14-320.jpg)