This document discusses various non-thyroid neck swellings including:
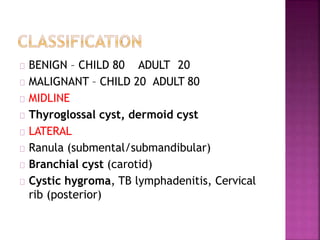
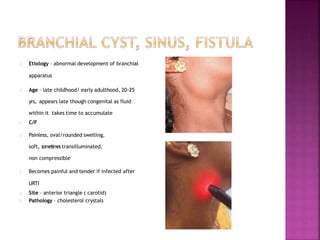
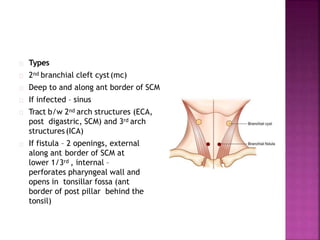
1. Benign cysts such as branchial cysts, dermoid cysts, and ranulas.
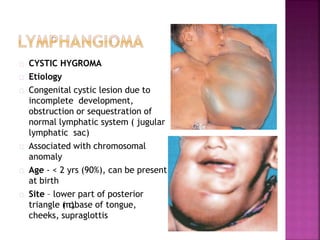
2. Inflammatory conditions including cystic hygroma and tuberculosis lymphadenitis.
3. Malignancies including lymphomas presenting as neck node enlargement and metastases from unknown primary cancers.
Diagnosis and treatment options are provided for each condition in brief.












































![benign neck disease [Autosaved].pptx orlhns](https://cdn.slidesharecdn.com/ss_thumbnails/benignneckdiseaseautosaved-241117151930-f0f5c123-thumbnail.jpg?width=640&height=640&fit=bounds)


















































