Downloaded 29 times

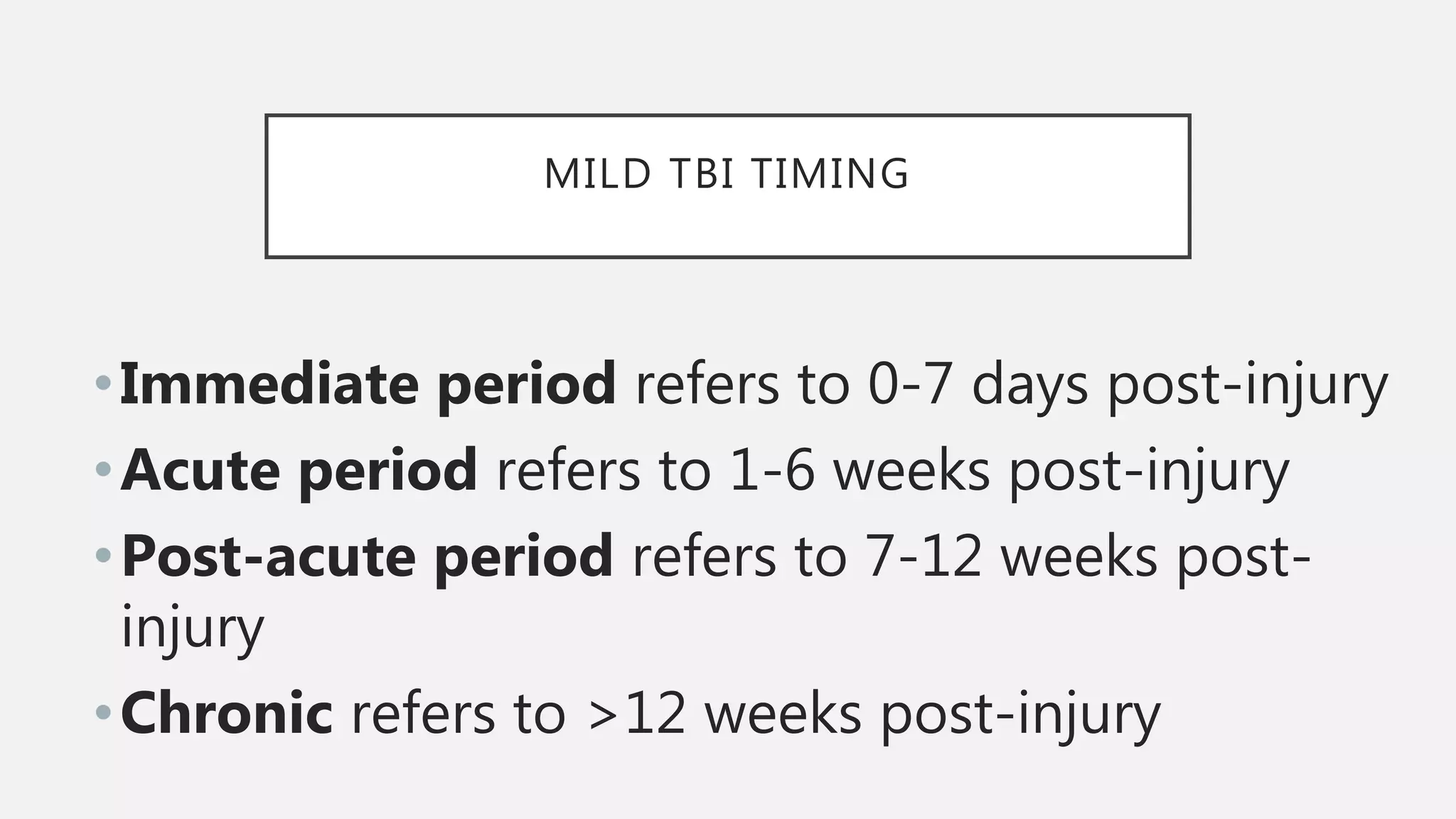



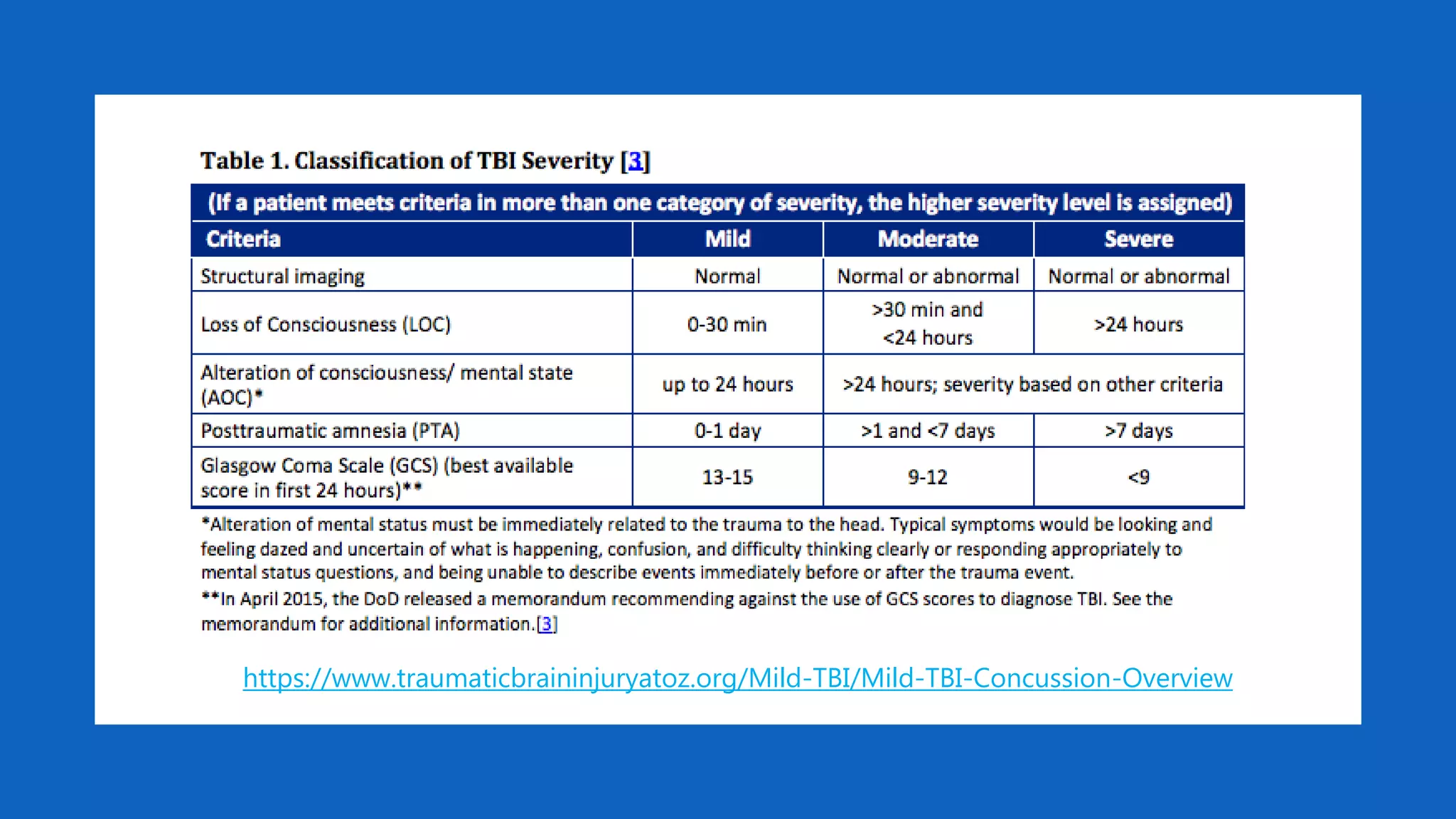




































The document discusses various aspects of traumatic brain injury (TBI), including its classification by time post-injury and the different types of related headaches and cognitive challenges. It highlights the role of interdisciplinary care in managing TBI symptoms, such as depression, mania, and the use of pharmacotherapy like antidepressants and psychostimulants. Additionally, it addresses the neuropsychological effects and treatment approaches for both acute and chronic TBI conditions.