Downloaded 548 times















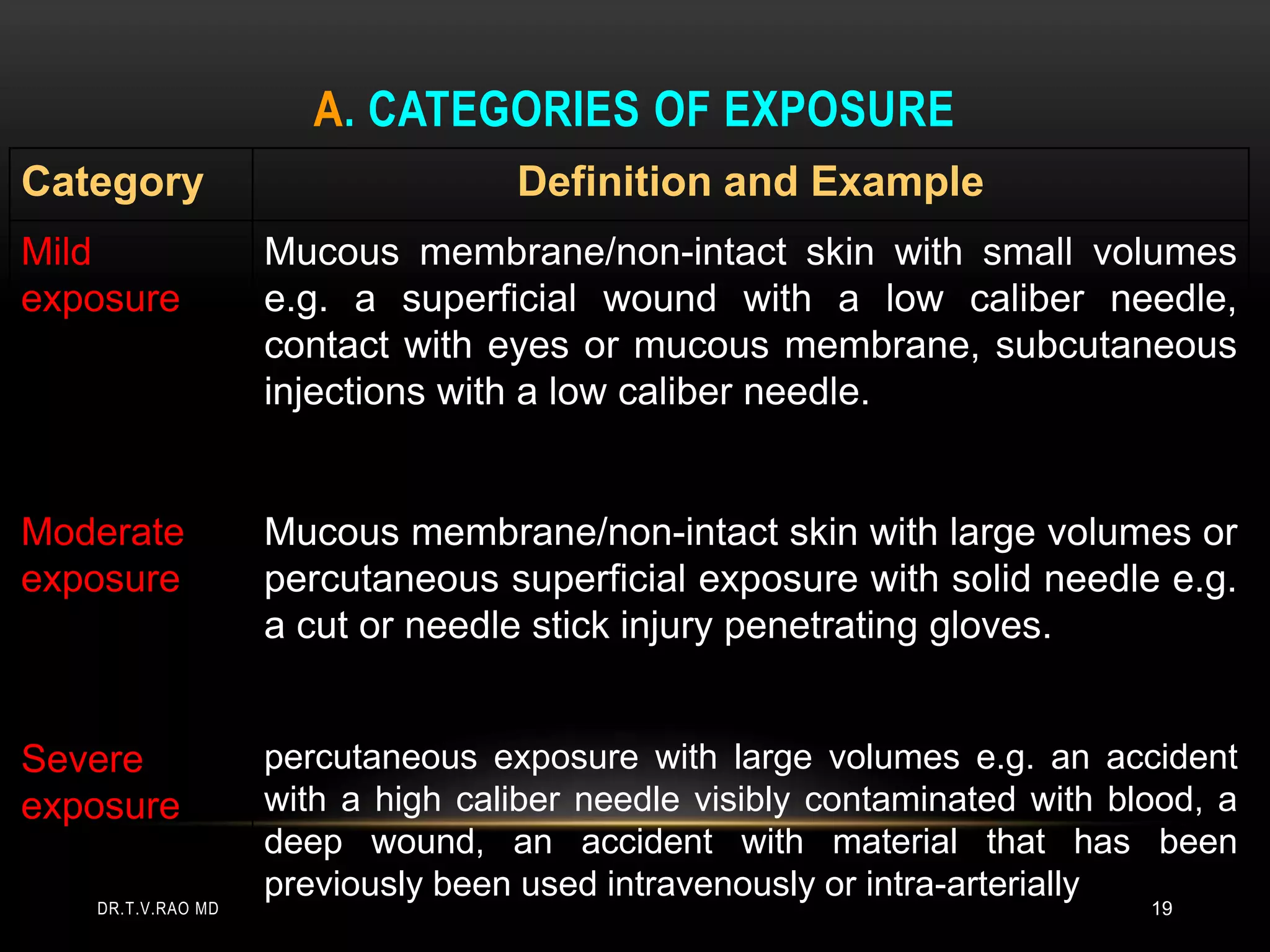













Nurse and doctors are most at risk of needlestick injuries which commonly occur during disposal. Recapping needles is a major risk factor. Such injuries can expose workers to Hepatitis B, Hepatitis C, and HIV. The risk of infection is highest for deep injuries involving visible blood. Proper sharps disposal, safety devices, and vaccination can help prevent injuries. Hospitals must provide post-exposure prophylaxis drugs according to guidelines to protect healthcare workers.



























![Sharp injuries and needle stick post exposure prophylaxis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/sharpinjuriesandneedlestickpostexposureprophylaxiscompatibilitymode-131231013025-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
























































