Downloaded 82 times





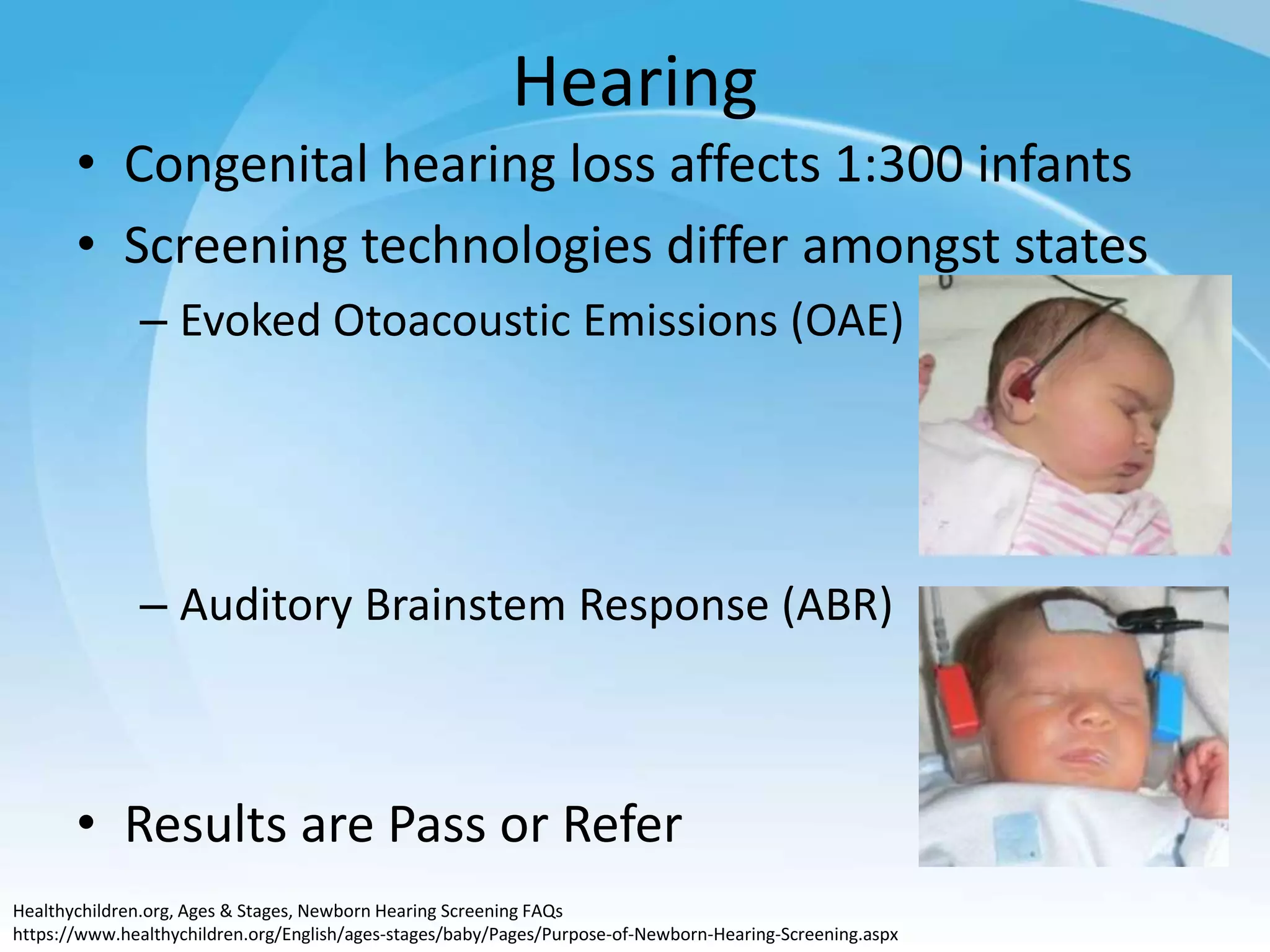


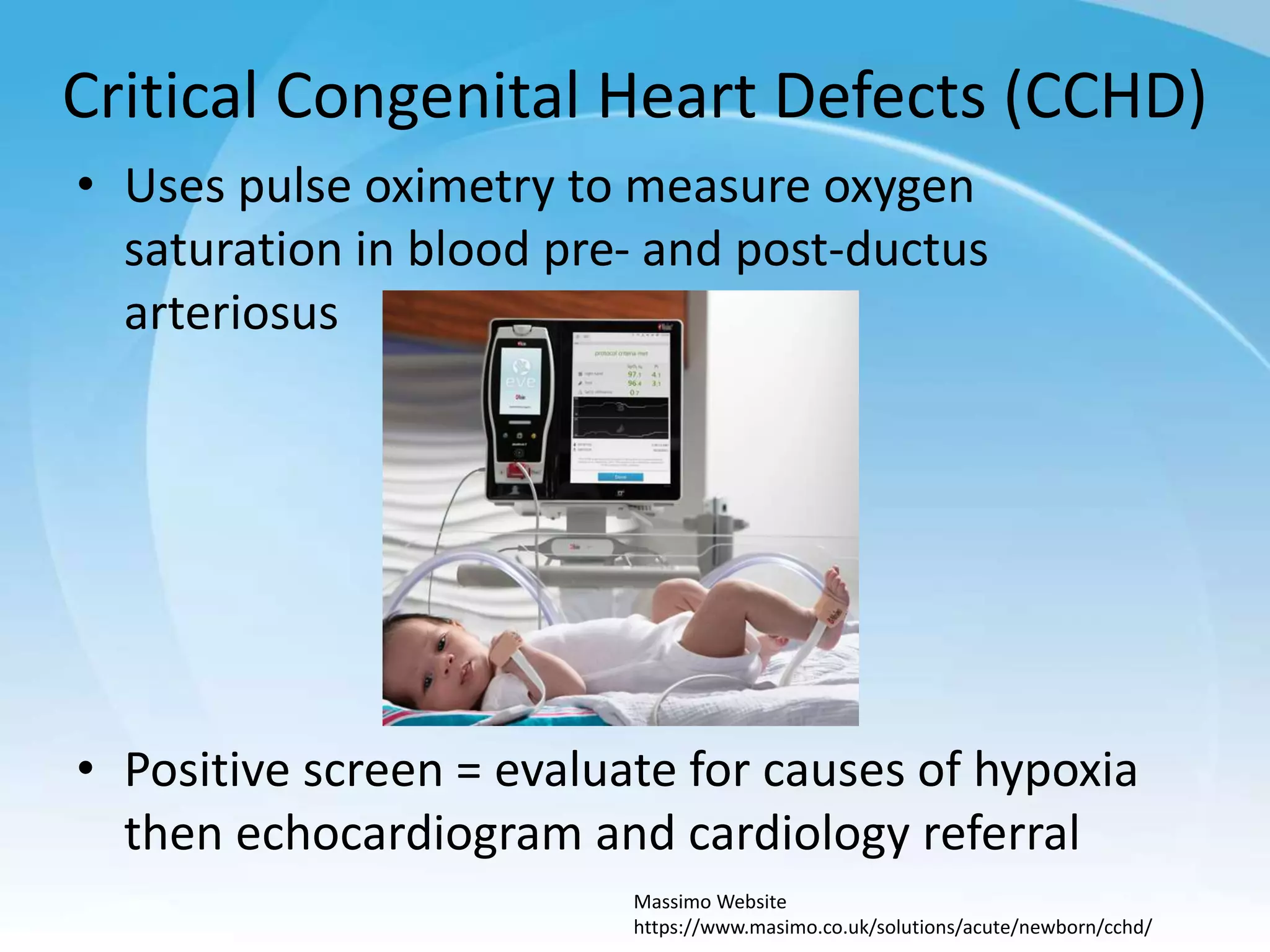



















Newborn screening involves testing newborns for treatable genetic and metabolic disorders through methods like dried bloodspot testing, hearing screening, and pulse oximetry. The goals are to identify at-risk newborns early before symptoms present, when treatment is most effective. Abnormal screening results require follow up diagnostic testing, education of families, and treatment if a condition is confirmed. Future directions may include expanded screening panels and genomic newborn screening, though these raise additional complex issues to consider.