4
INTRODUCTION
Epidemiology isa scientific and systemic study of distribution and
determinants (causes and risk factors) of health and disease related
states and their applications in the prevention, control, and management
of health-related problems.
It helps to plan and use appropriate strategies such as surveillance,
disease specific control, elimination and/or eradication strategies (such
as polio eradication and measles elimination)
In vaccine preventable diseases (VPDs), epidemiology plays a crucial role
to assess and monitor the burden of the diseases, surveillance methods,
immunization programs, plan out newer strategies and vaccine(s)
research.
5.
5
DEFINITIONS
Incidence: It isthe number of new cases occurring in a defined population
during a specified time period or duration.
Prevalence: It is the number of total cases (old and new) at a given point of
time (point prevalence) or in a specified period of time (period prevalence).
6.
6
DEFINITIONS
Immunogenicity: It isthe ability of the antigens to produce the antibodies.
It is also defined as the capacity of the vaccine to produce cell-mediated
and/or antibody- *mediated immunity and/or immunological memory.
Antibody Production
Immunogenicity Cell-Mediated Immunity
Immunological Memory
7.
7
DEFINITIONS
Seroconversion: It meansmore than or equal to four-fold increase in the antibody
titers from prevaccination to post vaccination level or detectable postvaccination
titer in a vaccinee who had no detectable antibody before vaccination.
.
8.
8
DEFINITIONS
Seroprotection: It impliesa state of protection from disease due to the presence
of a certain detectable level of antibodies in serum.
Vaccine efficacy: It is the ability of the vaccine to protect an individual under
experimental conditions.
Vaccine effectiveness: It is the ability of the vaccine to protect the community
and is the combination of vaccine efficacy and herd effect.
Herd effect: It is the protection offered to unvaccinated members when good
proportion (usually >85%) of the population is vaccinated. An effective vaccine is a
prerequisite for good herd effect.
9.
9
DEFINITIONS
Herd immunity: Itis the proportion of immune individuals in a
population. Individuals may acquire immunity following a disease or
immunization against that disease, e.g., all those who have had chickenpox
plus those who have acquired immunity because of varicella immunization
shall constitute the immune individuals in a given population.
Natural
Immunity
Herd Immunity
Vaccine-
Induced
Immunity
10.
10
DEFINITIONS
Vaccination: It isthe process of administering the vaccine which may or
may not evoke a protective immune response.
Immunization: It is the artificial and purposeful induction of specific
immune response by administering specific antigens to stimulate antibody
production.
12
INTRODUCTION
The firstuse the term vaccine was invented by Edward Jenner in
1796.
A vaccine is a biological preparation administered to stimulate an
individual’s immune system to develop adaptive immunity to a
pathogen
It prevents or ameliorate infectious diseases.
Choices of vaccine design are typically based on the fundamental
information about the microbes, such as how it infects cells and
how the immune system responds to it, as well as practical
considerations, such as regions of the world where the vaccine
14
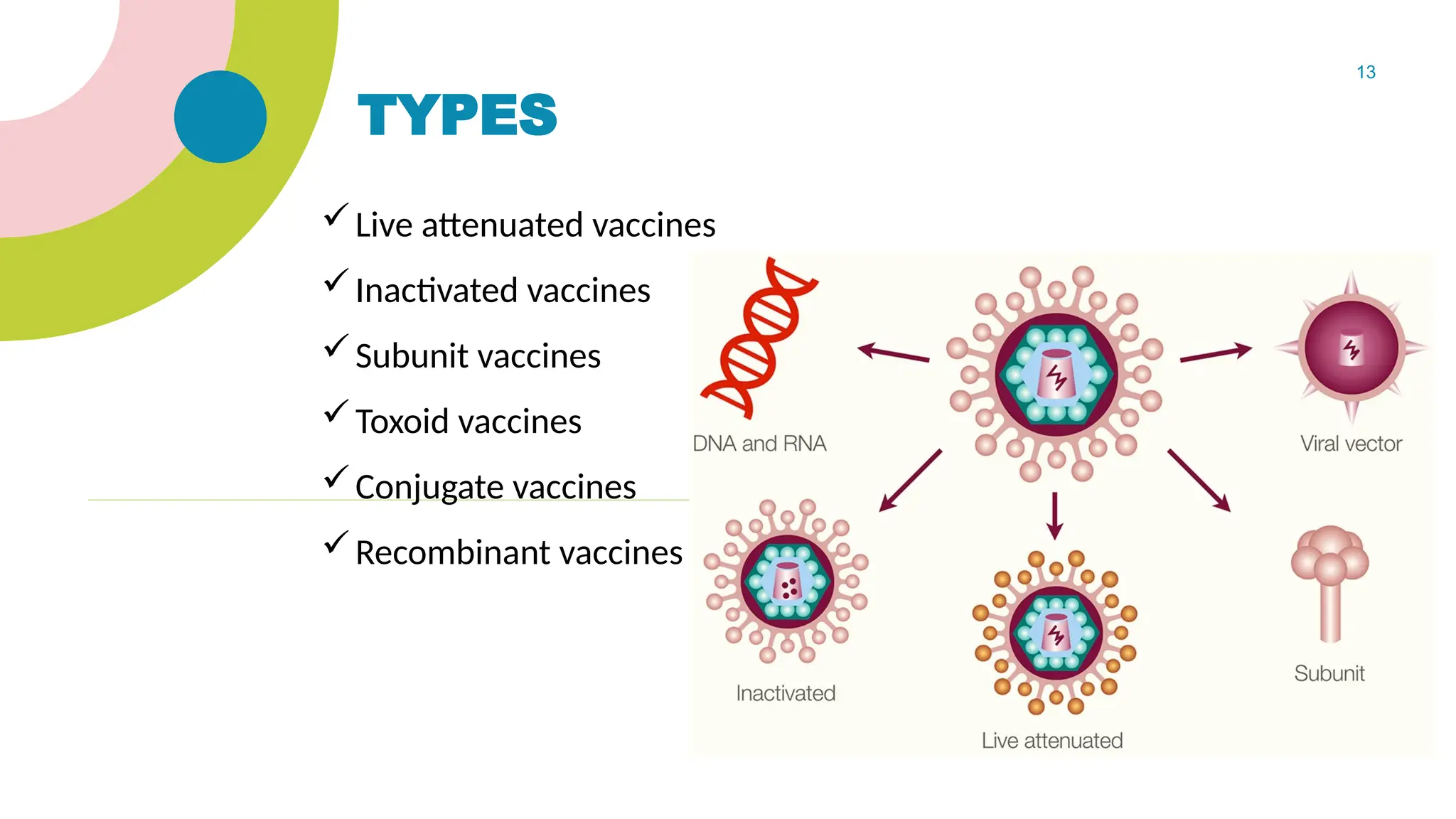
LIVE ATTENUATED VACCINES
Contains a version of the living microbe that has been weakened in the lab
Elicits strong cellular and antibody responses and often confer lifelong
immunity with only one or two doses.
Live vaccines are used to protect against: A) Measles, mumps, rubella
(MMR vaccine) B) Rotavirus C) Yellow fever D)Varicella E) BCG F) OPV
Live, attenuated vaccines are relatively easy to create for certain viruses
because they contain a small number of genes enabling scientists to readily
control their characteristics.
The live pathogen is attenuated by freezing, heating, dehydration and
exposure to radiation.
Contraindication - Immunocompromised
15.
15
INACTIVATED VACCINES
Producedby killing the disease-causing microbe with chemicals, heat,
or radiation
More stable and safer than live vaccines: The dead microbes can’t
mutate back to their disease-causing state
Inactivated vaccines usually don’t provide immunity (protection) that’s
as strong as live vaccines. So you may need several doses over time
(booster shots) in order to get ongoing immunity against diseases.
Inactivated vaccines are used to protect against:
A) Hepatitis A B) Flu C) Polio(IPV) D) Rabies
16.
16
SUBUNIT VACCINES
Vaccinesinclude only the antigens that best stimulate the immune
system.
Subunit vaccines can contain anywhere from 1 to 20 or more antigens.
A) growing the microbe in the laboratory and then using chemicals to
break it
apart and gather the important antigens. B) Manufacturing the antigen
molecules from the microbe using recombinant DNA technology. Vaccines
produced this way are called “recombinant subunit vaccines.”
Hepatitis B , Human papilloma virus vaccines, Acellular pertusis
Subunit vaccines contain only the essential antigens and not all the other
17.
17
TOXOID VACCINES
Vaccinesmade from detoxified toxin.
Inactivated toxins by treating them with formalin, a solution of
formaldehyde and sterilized water.
When the immune system receives a vaccine containing a harmless
toxoid, it learns how to fight off the natural toxin. The immune system
produces antibodies that lock onto and block the toxin.
These are safe because they cannot cause the disease they prevent and
there is no possibility of reversion to virulence.
Diphtheria, Tetanus vaccines
The vaccine antigens are not actively multiplying and do not spread to
unimmunized individuals.
18.
18
CONJUGATE VACCINES
Thereare some bacteria that are coated with sugar molecules
calcoating.y saccharide, which are the antigens.
A part of the sugar coating and use it in the vaccine so that the body
creates immunity to the sugar coating
These conjugate vaccines also have antigens or toxoids, often from the
same bacteria, linked to the sugar molecules.
The vaccine that protects against Haemophiles influenzae type B (Hib),
pneumococcal, meningococcal & Vi- typhoid vaccines - conjugate
vaccine.
19.
19
RECOMBINANT VACCINES
Vectorvaccines are experimental vaccines similar to DNA vaccines, but
they use an attenuated virus or bacterium to introduce microbial DNA to
cells of the body.
“Vector” refers to the virus or bacterium used as the carrier.
Use of certain harmless or attenuated viruses to insert portions of the
genetic material from other microbes into them.
The carrier viruses then ferry that microbial DNA to cells, provoking an
immune response.
COVID – 19 {Covishield}
Recombinant vector vaccines closely mimic a natural infection and
therefore do a good job of stimulating the immune system.
20.
20
It isaccomplished by administration of preformed antibodies to
provide immediate protection
These antibodies are derived from pooled plasma of adults by an
alcohol fractionation procedure
Primarily consists of IgG with trace amounts of IgA and IgM
Large no of donors needed
Used in
• Replacement therapy in congenital or acquired immunodeficiency
disorders
• Leukemia children, who can develop life-threatening complications-
measles, pox
• Rabies, hepatitis B, Tetanus and measles where time does not permit
adequate protection
22
INTRODUCTION
Immunization schedulesare the basic framework for the delivery of
vaccines and immunization to the individuals and the community. A
well-planned immunization schedule should be epidemiologically
relevant, immunologically effective, operationally feasible, and socially
acceptable.
Various factors include
(1) Epidemiology of the disease
(2) Age-specific morbidity and mortality
(3) Vaccine effectiveness
(4) Risks of vaccine-related adverse events
(5) Cost-effectiveness
23.
23
UNIVERSAL IMMUNIZATION PROGRAM
The Expanded Program of Immunization (EPI) was launched by WHO
in 1974. It was launched in India in 1978 and was renamed as
Universal Immunization Program (UIP) in 1985 to achieve target
immunization goals in a phased and planned manner.
The UIP targeted infants below 1 year of age against target diseases
as well as pregnant women who were to be immunized against
tetanus.
The aim was to achieve 100% coverage of all pregnant women and at
least 85% coverage of infants.
Measles vaccine became a part of UIP and the schedule was devised
to protect infants and children from six major VPDs namely
tuberculosis, diphtheria, pertussis, tetanus,
24.
24
COMPONENTS OF UIP
Theobjectives and focus of UIP included:
• Rapidly increasing immunization coverage and reduction of mortality
and morbidity due to six VPDs.
• Improve the quality of service.
• Establish a reliable cold chain system till health facility level.
• Phased implementation-all districts to be covered by1989-1990.
• Introduce a district-wise system for monitoring and evaluation.
• Achieve self-sufficiency in vaccine production and manufacture of cold
chain equipment
childhood immunization received a further thrust and many years later
in 2012, India declared the year as "Intensification of Routine
Immunization in India" and WHO removed India from the list of polio
25.
25
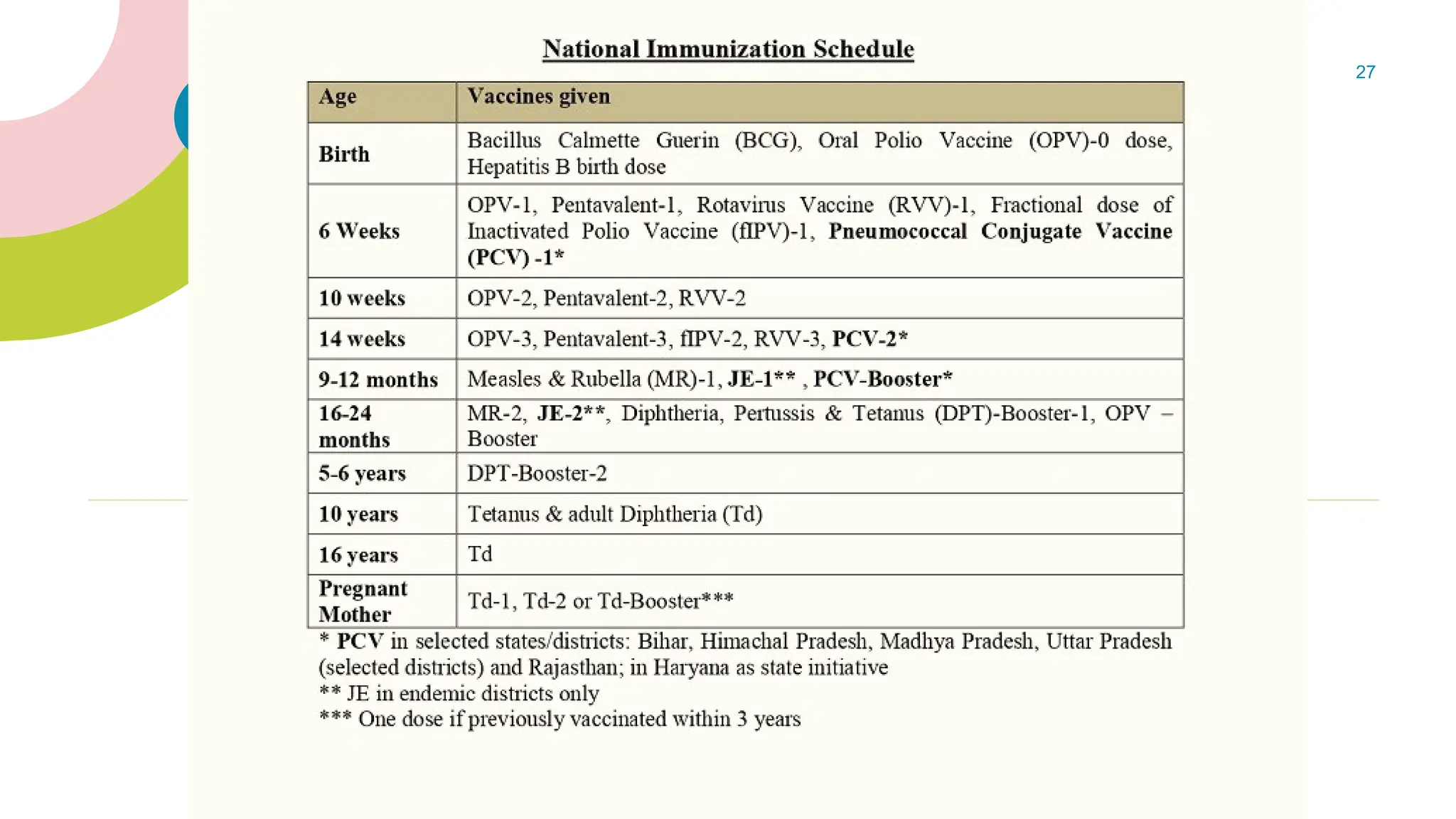
NATIONAL IMMUNIZATION PROGRAM
The epidemiological patterns of the diseases are often different in
different countries and thus the immunization schedule of one country
often differs from another.
Even within the states, a few disease patterns may vary, e.g., vaccine for
Japanese encephalitis is used under NIP in North Eastern states, where
this disease is endemic.
Besides, childhood immunization is a dynamic and evolving scientific
process, thus necessitating the addition of newer vaccines in NIP.
The examples of such recent introduction of vaccines under NIP include
PCV and rotavirus vaccines, which are known to prevent morbidity and
mortality from two leading causes of under <5 mortality namely
childhood pneumonia and diarrhea.
26.
26
NIP - Contd
Disease patterns and immunization needs may continue to change in
future as more information on diseases becomes available and the
development of newer vaccines continues to take place.
Strategies such as catch-up immunization and supplementary
immunization days (e.g., polio ravivaar) are additional tools in NIP.
Hence, there is a constant need to revise the recommendations about
the vaccines and their scheduling. Besides with the eradication of
poliomyelitis from India, the need to address the potential safety issues
with oral polio vaccine (OPV) was prioritized, leading to introduction of
fractional doses of inactivated polio vaccine (IPV) under NIP.
28
ASSESS PATIENT FORFITNESS FOR
IMMUNIZATION AND PRESCRIBE AN AGE-
APPROPRIATE IMMUNIZATION SCHEDULE
At every healthcare visit, child's vaccination status must be reviewed to avoid any
missed opportunity for vaccination.
Look out for the general wellbeing of the child and ask the parents if the child has
any complaints and assess accordingly. Ask for any relevant past history of febrile
seizures.
Look out for any contraindications and precautions even if the child has received
the vaccine earlier.
Minor illnesses such as mild fever, cold and/or diarrhea are not a contraindication
to the use of vaccine and the vaccination should not be delayed to a further date.
Perform a quick examination and assessment of the child before actual
administration of the vaccine(s).
29.
29
SUMMARY
In vaccinepreventable diseases (VPDs), epidemiology plays a crucial role to assess and monitor the burden of
the diseases, surveillance methods, immunization programs, plan out newer strategies, and vaccine(s) research.
Vaccines are a preparation which contain live (attenuated) or inactivated organisms (such as bacteria or viruses)
or fractions (e.g., subunit, polysaccharides, and toxoids) thereof, administered to induce active immunity and
prevent infectious disease or its sequels.
An immunization schedule should be epidemiologically relevant, immunologically effective, operationally
feasible, and socially acceptable.
Vaccines are recommended at an earliest age when there is a significant risk of disease/complications and at
which al protective immunological response is expected.
Well child visits provide excellent opportunities to assess the immunization status of every child and to avoid
any missed opportunities for immunization