Outline
• Key Definitions
–Immunisation vs. Vaccination
– Objectives of vaccination
• Vaccines
– Definition of a vaccine
– Properties of an ideal vaccine
– Overview of types and examples of vaccines
– Components of different vaccines
– Technologies applied to produce vaccines
– Examples of vaccines
• Presentations of Vaccines
– Monovalent vs. Polyvalent (combination) vaccines
– Liquid
– vs. Freeze-dried vaccines (Measles, yellow fever, HiB and BCG)
8.
How vaccines work?
•Vaccines use the knowledge of the
immune system to mimic infection,
generate immunologic memory, and
prepare the body for future infections.
• An ideal vaccine
– provides lifelong immunity from disease
– protects against multiple strains of the same
disease
– it is safe, inexpensive, stable
– preferably not administered via injection (not
always possible)
9.
• The mainobjective of the vaccination
schedule is to protect individuals from
disease by providing immunity before
they acquire disease.
• To understand how vaccines provide
protection, it is important to understand the
essential components that compose the
immune system and how the immune
system generates a response to
perceived pathogens.
10.
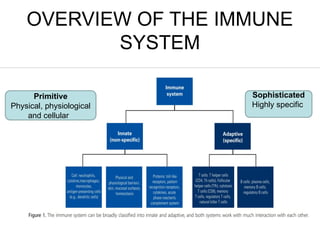
OVERVIEW OF THEIMMUNE
SYSTEM
Primitive
Physical, physiological
and cellular
Sophisticated
Highly specific
11.
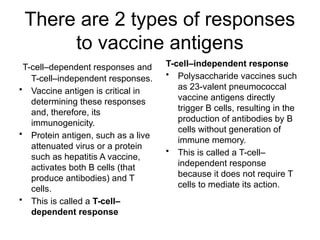
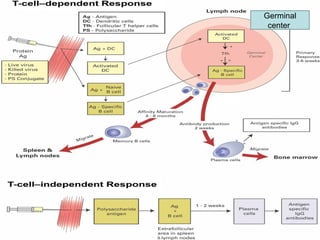
There are 2types of responses
to vaccine antigens
T-cell–dependent responses and
T-cell–independent responses.
• Vaccine antigen is critical in
determining these responses
and, therefore, its
immunogenicity.
• Protein antigen, such as a live
attenuated virus or a protein
such as hepatitis A vaccine,
activates both B cells (that
produce antibodies) and T
cells.
• This is called a T-cell–
dependent response
T-cell–independent response
• Polysaccharide vaccines such
as 23-valent pneumococcal
vaccine antigens directly
trigger B cells, resulting in the
production of antibodies by B
cells without generation of
immune memory.
• This is called a T-cell–
independent response
because it does not require T
cells to mediate its action.
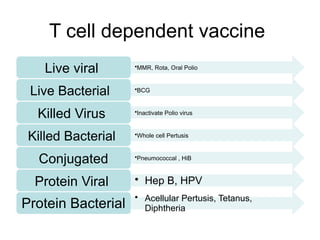
T cell dependentvaccine
Live viral •MMR, Rota, Oral Polio
Live Bacterial •BCG
Killed Virus •Inactivate Polio virus
Killed Bacterial •Whole cell Pertusis
Conjugated •Pneumococcal , HiB
Protein Viral • Hep B, HPV
Protein Bacterial
• Acellular Pertusis, Tetanus,
Diphtheria
14.
T cell independentVaccines
Polysaccharide vaccines
Salmonell
a Typhoid
Meningoc
occal
Pneumoc
occal
PCV 23
15.
• Vaccines containthe same antigens (or parts of
antigens) that cause diseases. For example, measles
vaccine contains measles virus.
• But the antigens in vaccines are either killed, or
weakened to the point that they don’t cause disease.
• However, they are strong enough to make the immune
system produce antibodies that lead to immunity.
• In other words, a vaccine is a safer substitute for a
child’s first exposure to a disease.
• The child gets protection without having to get sick.
Through vaccination, children can develop immunity
without suffering from the actual diseases that vaccines
prevent.
16.
More Facts
• Newbornbabies are immune to many diseases
because they have antibodies they got from their
mothers. However, this immunity goes away during
the first year of life.
• If an unvaccinated child is exposed to a disease germ,
the child’s body may not be strong enough to fight the
disease.
• Before vaccines, many children died from diseases
that vaccines now prevent, such as whooping cough,
measles, and polio.
• Those same germs exist today, but because babies
are protected by vaccines, we don’t see these
diseases nearly as often.
17.
Immunizing individual childrenalso helps to protect the
health of our community, especially those people who
cannot be immunized (children who are too young to be
vaccinated, or those who can’t receive certain vaccines
for medical reasons), and the small proportion of people
who don’t respond to a particular vaccine (herd
immunity) .
Diseases that are vaccine-preventable have a costly
impact, resulting in doctor’s visits, hospitalizations, and
premature deaths. Sick children can also cause parents
to lose time from work.
18.
The main objectiveof the vaccination schedule
• is to protect individuals from
disease by providing immunity before they
acquire disease.
• Long-term immunity is important in determining
the effectiveness of the immunization
schedule.
• Important factors in determining the
immunization schedule:
• Short-term protection
• local prevalence and incidence
• disease epidemiology
• safety
• programmatic aspects (including number of doses, funding,
organization, and cost)
19.
IMMUNISATION
• Two FORMSof immunisation
– Passive immunisation
• Natural passive immunisation = transplacental or colostral
transfer of antibodies from the mother to the baby
• Artificial passive immunisation = intramuscular inoculation of
immunolobulin [IG])
– Active immunisation
• Natural - following resolution of natural infection
• Artificial - direct inoculation of a vaccine, the process is called
vaccination
• Important to note that:
– Immunisation is NOT synonymous to vaccination
– Vaccination is another form of immunisation
– Vaccination ONLY involves the use of a vaccine
Science of controlling and preventing infectious diseases
20.
WHAT IS AVACCINE?
Modified from Canadian residents vaccine training program
A suspension of live attenuated (replicating) or killed (non-replicating)
microorganisms* or subunit / fractions* (non-replicating) thereof (i.e.
purified protein subunits, polysaccharides, or split virions) that are
administered (IM, SC, ID, Mucosal, or Oral), for the prevention or
treatment of infectious diseases
*subunits or fractions from virus, bacterium, fungus, or parasite
(Antigen)
Vaccines can be classified using different parameters
21.
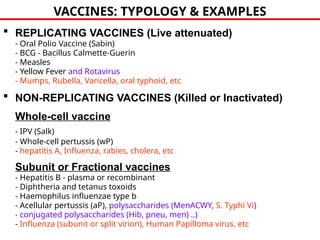
VACCINES: TYPOLOGY &EXAMPLES
REPLICATING VACCINES (Live attenuated)
- Oral Polio Vaccine (Sabin)
- BCG - Bacillus Calmette-Guerin
- Measles
- Yellow Fever and Rotavirus
- Mumps, Rubella, Varicella, oral typhoid, etc
NON-REPLICATING VACCINES (Killed or Inactivated)
Whole-cell vaccine
- IPV (Salk)
- Whole-cell pertussis (wP)
- hepatitis A, Influenza, rabies, cholera, etc
Subunit or Fractional vaccines
- Hepatitis B - plasma or recombinant
- Diphtheria and tetanus toxoids
- Haemophilus influenzae type b
- Acellular pertussis (aP), polysaccharides (MenACWY, S. Typhi Vi)
- conjugated polysaccharides (Hib, pneu, men) ..)
- Influenza (subunit or split virion), Human Papilloma virus, etc
23.
PROPERTIES OF ANIDEAL VACCINE
• Safe – revert to virulence, toxicity of killed vaccine
• Immunogenic
– Host responds with appropriate immunity
• Effective duration
• Non-immunosuppressive
• Cost vs benefit
– monetary and risk with use
– recipient and population
– e.g. killed cells inexpensive – low benefits bec of S/E
• Relative risk of vaccine vs infection
24.
History of theNational Immunization
Programme in Zimbabwe
• The EPI was established in 1974 through the resolution WHA27.57
to build on the success of the global smallpox eradication
programme.
• The Zimbabwe expanded program on immunization, (ZEPI)
established as a component of primary health care at independence
in 1980
• Focus on building a sustainable immunization system to protect
children against common vaccine-preventable diseases:
Initially 6 vaccines: diphtheria, tetanus, pertussis, poliomyelitis, TB,
and measles.
Other vaccines have since been added: HIB, HBV, PCV, ROTA, MR.
HPV, Typhoid (TCV)
Pipeline: Hep B birth dose
Immunization of pregnant women and WCBA: preventing maternal
tetanus and newborn infants from neonatal tetanus.
25.
Tuberculosis
• Bacterial infection-
mycobacteriumtuberculosis
• Droplet infection, S & S varies
• Vaccine –Bacille Caimette
Guerin (BCG),many strains
• Live attenuated, freeze dried
• Reduces morbidity and
mortality from TB in infants,
meningitis, miliary TB
• At birth, intradermal Right
arm-insertion of deltoid
muscle
• acute diseasecaused by exotoxin
producing
Corynebacterium diphtheriae
• highly contagious disease
• humans are the only source of infection
• transmitted via respiratory aspiration
and exudate from infected skin lesions1
• typically a disease of upper respiratory
tract
mortality is highest in young and elderly1,2
adapted from Diphtheria vaccine,
WER N3 Jan 20, 2006; 81 pp.24-32
Diphtheria
28.
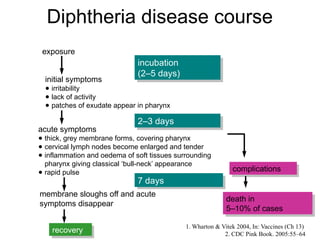
Diphtheria disease course
recovery
deathin
5–10% of cases
exposure
initial symptoms
● irritability
● lack of activity
● patches of exudate appear in pharynx
acute symptoms
● thick, grey membrane forms, covering pharynx
● cervical lymph nodes become enlarged and tender
● inflammation and oedema of soft tissues surrounding
pharynx giving classical ‘bull-neck’ appearance
● rapid pulse
membrane sloughs off and acute
symptoms disappear
incubation
(2–5 days)
2–3 days
7 days
complications
1. Wharton & Vitek 2004, In: Vaccines (Ch 13)
2. CDC Pink Book. 2005:55–64
29.
Diphtheria
prevention
(Inactivated
Toxin)
• vaccines basedon diphtheria toxoid (modified
toxin)
inducing protective anti-diphtheria toxin
antibodies
• DTPw part of EPI since 1974; from 1980-2000
>90% reduction in the number of reported
cases
• following priming (3 im doses generally at
6,10,14
weeks) protection lasts for +/- 10 years;
boosters at
2nd year and to 4-6 year olds if resources
permit
• immunity maintenance through exposure to
toxigenic
C. diphtheriae in areas of low vaccination
coverage;
if coverage is high, because of low level of
natural
boosting there is a need for booster
vaccinations
adapted from Diphtheria vaccine, WER N3 Jan 20,
2006; 81 pp.24-32
30.
Etiology – Characteristics
TbbTtbbtteTttttttt
•Infectious bacterial disease caused due to toxin produced by
anaerobic bacterium (Clostridium tetani)
– Highly potent neurotoxin (tetanospasmin)
– It is a single polypeptide chain
– Neurotropic
• Extremely potent
– Estimated human lethal dose is 2.5 ng/kg
– Once inside the neuron it cannot be neutralized by tetanus antotoxin
• Disease may affect any age group
– Mainly newborns in developing countries ; unclean delivery & Poor
post natal hygiene ( poor cord care practices)
– Maternal Tetanus –unsafe abortion; unclean delivery
– Elderly
Tetanus
31.
Neonatal
tetanus -
Disease •Initial sign – clenching of jaws (lock-jaw)
• Spasm of facial muscles – risus sardonicus
• Gradual spasm of all muscles, arching back,
clenched fists, followed by convulsions
• Spasm of breathing muscles lead to suffocation
• Infection of umbilical stump
• Incubation period: 1 day – 3 months
(normally 3 days to 3 weeks)
• Intense disease for 4 weeks, then
subsides
• Mortality directly proportional to the
quality of care given (eg ventilation)
10–70% but with best care, age and
general health of the patient mortality
10-20%
32.
TT vaccine
presentations
Single toxoid(TT)
Combined with diphtheria toxoid (DT) or low-
dose diphtheria toxoid (Td)
Combined with diphtheria and pertussis
vaccines (DTwP, DTaP, dTaP or dTaP)
33.
Tetanus
Toxoid
vaccine I
Interval betweendoses is 4 weeks
• For perinataly infected children response to TT was adequate for 2 years of life
• In HIV infected adults ab response is less than non HIV infected adults but concentration of ab is
substantial
Longer interval may provide increased
magnitude and duration of protection (not
reason to delay schedule)
Efficacy in most clinical trials is 80-100%
Response to vaccination is similar between
malaria infected pregnant mothers and non
malaria infected adults
Antibody response to TT in children with AIDS
is impaired like other vaccines
34.
Pertussis
Bordetella pertussis, highlyinfectious
Severe cough often with whoop, cyanosis and vomiting-6-8wks
Young infants-apnoeic spells
3 stages; catarrhal, paroxysmal, convalescent
Treatment erythromycin
Pentavalent and 18months booster. 5years not given
35.
Pertussis disease course
1.CDC Pink Book. 2005:75–88
2. Linnemann Jr 2003, In: Oxford Textbook of Medicine (Ch 7.11.14)
3. Mortimer Adv Pediatr Infect Dis1990;5:1–33
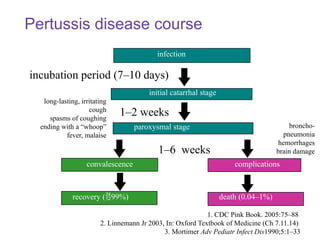
incubation period (7–10 days)
convalescence complications
infection
paroxysmal stage
initial catarrhal stage
1–2 weeks
1–6 weeks
recovery (99%) death (0.04–1%)
long-lasting, irritating
cough
spasms of coughing
ending with a “whoop”
fever, malaise
broncho-
pneumonia
hemorrhages
brain damage
36.
1. CDC PinkBook. 2005:75–88
2. Mortimer Adv Pediatr Infect Dis
1990;5:1–33
3. Wortis et al. Pediatrics 1996;97:607–12
Pertussis
complications
• secondary respiratory infections (e.g.
pneumonia)1,2
• consequences of severe coughing;
conjunctivitis, nose bleeds, hernias,
atelectasia …
• CNS (from minor convulsions to
coma/ permanent brain damage)
• 87% deaths occur in infants
aged <1 year3
Contraindications
to wP vaccination
Neurologicillness due to vaccination
Persistent unconsolable screaming for 3 or more hours
Hypotonic hyporesponsive episode
Temperature of 40.5 C or >
Anaphylaxis
Febrile illness - defer
Evolving neurologic disease - defer
Acellular pertussis (aP) prefered
39.
Poliomyelitis
Viral, faeco- oraltransmission
Fever followed by AFP
Incubation period 8-12days
Paralytic occurs 0.1%
Suspected AFPs - 2 stool specimens 24-48hrs apart
Supportive management
40.
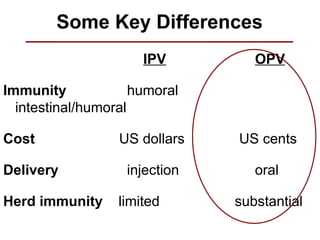
Some Key Differences
IPVOPV
Immunity humoral
intestinal/humoral
Cost US dollars US cents
Delivery injection oral
Herd immunity limited substantial
41.
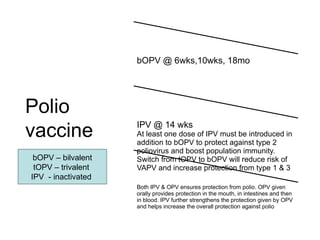
Polio
vaccine
bOPV @ 6wks,10wks,18mo
IPV @ 14 wks
At least one dose of IPV must be introduced in
addition to bOPV to protect against type 2
poliovirus and boost population immunity.
Switch from tOPV to bOPV will reduce risk of
VAPV and increase protection from type 1 & 3
Both IPV & OPV ensures protection from polio. OPV given
orally provides protection in the mouth, in intestines and then
in blood. IPV further strengthens the protection given by OPV
and helps increase the overall protection against polio
bOPV – bilvalent
tOPV – trivalent
IPV - inactivated
42.
Measles
Disease
• Acute viraldisease - Highly
infectious
• Transmission - via respiratory
secretions or aerosols
• Viral replication & dissemination
of virus into different organs
• Classic manifestations (Fever,
Maculopapular rash, the 3C:
Cough, Coryza, Conjunctivitis;
Kopliks spots)
• Mortality rate - 0.1 – 10%;Up to
30% in humanitarian
emergencies (Risk increases
with age, malnutrition, other
cause of impaired immunity)
43.
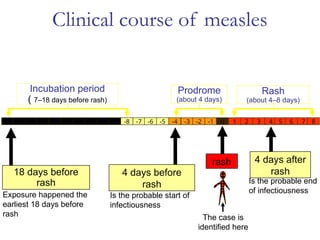
Clinical course ofmeasles
Incubation period
( 7–18 days before rash)
18 days before
rash
Exposure happened the
earliest 18 days before
rash
4 days before
rash
Is the probable start of
infectiousness
Prodrome
(about 4 days)
-18 -17 -16 -15 -14 -13 -12 -11 -10 -9 -8 -7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8
4 days after
rash
Is the probable end
of infectiousness
Rash
(about 4–8 days)
rash
The case is
identified here
44.
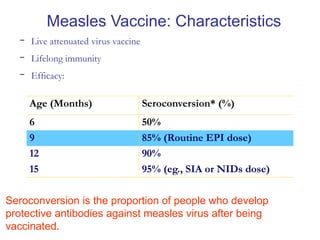
- Live attenuatedvirus vaccine
- Lifelong immunity
- Efficacy:
Age (Months) Seroconversion* (%)
6 50%
9 85% (Routine EPI dose)
12 90%
15 95% (eg., SIA or NIDs dose)
Seroconversion is the proportion of people who develop
protective antibodies against measles virus after being
vaccinated.
Measles Vaccine: Characteristics
45.
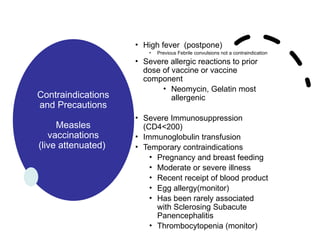
Contraindications
and Precautions
Measles
vaccinations
(live attenuated)
•High fever (postpone)
• Previous Febrile convulsions not a contraindication
• Severe allergic reactions to prior
dose of vaccine or vaccine
component
• Neomycin, Gelatin most
allergenic
• Severe Immunosuppression
(CD4<200)
• Immunoglobulin transfusion
• Temporary contraindications
• Pregnancy and breast feeding
• Moderate or severe illness
• Recent receipt of blood product
• Egg allergy(monitor)
• Has been rarely associated
with Sclerosing Subacute
Panencephalitis
• Thrombocytopenia (monitor)
46.
Hepatitis
B
• HBV
• Transmission-vertical,perinatal,
horizontal,parenteral and sexual
• Long-term HCC and Cirrhosis
particularly for vertical
transmission
• Plasma derived and DNA
recombinant vaccine
• 90% efficacy
• For ZEPI part of Pentavalent -
birth dose still under consideration
47.
HPV
(Human Papilloma
Virus)
• Pastdecade, two
prophylactic HPV vaccines,
– Cervarix® - bivalent
– Gardasil®) both the quadri-
valent and 9 – valent
• licensed globally
• for the prevention of
infection and precancerous
cervical lesions caused by
HPV (Meites, 2016).
48.
HPV
• Clinical trialshave shown that a
three dose HPV vaccination
schedule is 100% efficacious in
preventing high grade cervical
intraepithelial neoplasia (CIN3+)
and adenocarcinoma in situ (AIS)
in HPV naive females (Munoz,
2010)(Apter, 2015).
• Concurrently, this preventive
treatment was also shown to have
an acceptable safety profile and
sustained immunogenicity
49.
Adverse
Events
Following
HPV
Immunization
• 53 parents,5.6 % reported
[Beitbridge 7.5%,
Marondera 3.7%)
– Dizziness, fever, headache,
nausea, vomiting, fatigue,
rash and swelling, pain at
injection site
• Mostly (57% BB, 72%
MDA) were mild and/or
shortlived…needed no
treatment, or gave pain
killer,
50.
Haemophilus
influenzae
type B
Subunit
(purified antigen)
•Important cause of bacterial
meningitis in childhood
• Pneumonia, epiglotitis,
arthritis, otitis media,
septicemia etc
• Conjugate vaccine
• Combination vaccine
(Pentavalent)
• Efficacy 95-100%
• Herd immunity
51.
Rotavirus
• Leading causeof severe
gastroenteritis in infants
and young children
• Seasonal -2 peaks in
Zimbabwe
• Two vaccines, Rotarix(2
doses) and Rotateq( 3
doses)
• Zimbabwe use Rotarix oral
vaccine at 6 weeks and
10weeks
• Contraindicated after 32
weeks-Intusussception
52.
Pneumococcal
• Diseases causedby
Streptococcus
pneumoniae are a
major public health
problem worldwide.
• Pnemonia,
meningitis,
bacteraemia, otitis
media, sinusitis and
bronchitis
• Types of vaccine……
53.
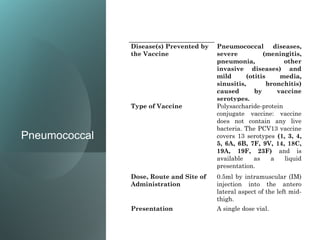
Pneumococcal
Disease(s) Prevented by
theVaccine
Pneumococcal diseases,
severe (meningitis,
pneumonia, other
invasive diseases) and
mild (otitis media,
sinusitis, bronchitis)
caused by vaccine
serotypes.
Type of Vaccine Polysaccharide-protein
conjugate vaccine: vaccine
does not contain any live
bacteria. The PCV13 vaccine
covers 13 serotypes (1, 3, 4,
5, 6A, 6B, 7F, 9V, 14, 18C,
19A, 19F, 23F) and is
available as a liquid
presentation.
Dose, Route and Site of
Administration
0.5ml by intramuscular (IM)
injection into the antero
lateral aspect of the left mid-
thigh.
Presentation A single dose vial.
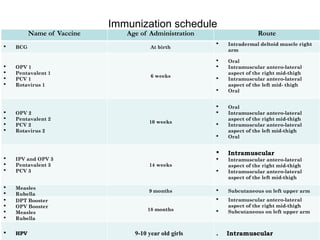
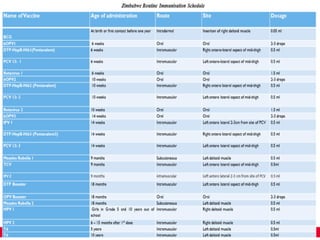
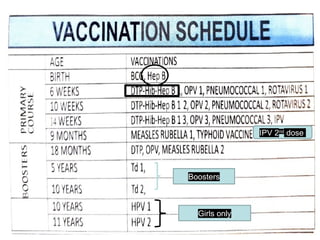
Immunization schedule
Name ofVaccine Age of Administration Route
BCG At birth
Intradermal deltoid muscle right
arm
OPV 1
Pentavalent 1
PCV 1
Rotavirus 1
6 weeks
Oral
Intramuscular antero-lateral
aspect of the right mid-thigh
Intramuscular antero-lateral
aspect of the left mid- thigh
Oral
OPV 2
Pentavalent 2
PCV 2
Rotavirus 2
10 weeks
Oral
Intramuscular antero-lateral
aspect of the right mid-thigh
Intramuscular antero-lateral
aspect of the left mid-thigh
Oral
IPV and OPV 3
Pentavalent 3
PCV 3
14 weeks
Intramuscular
Intramuscular antero-lateral
aspect of the right mid-thigh
Intramuscular antero-lateral
aspect of the left mid-thigh
Measles
Rubella
9 months Subcutaneous on left upper arm
DPT Booster
OPV Booster
Measles
Rubella
18 months
Intramuscular antero-lateral
aspect of the right mid-thigh
Subcutaneous on left upper arm
HPV 9-10 year old girls . Intramuscular
Premature Babies
• Babiesshould get their vaccines on time
• On their chronological age and not their
gestational age
• If baby is 30 weeks gestation 2kg and
weighs 2.5kg at 6 weeks vaccination
should be given
• Do not wait for baby to get to 3 kg before
vaccines are give
Take home message
•Vaccines prevent infection and childhood
diseases
• Know your local epidemiology of illness
• Try and vaccinate children at every
possible encounter
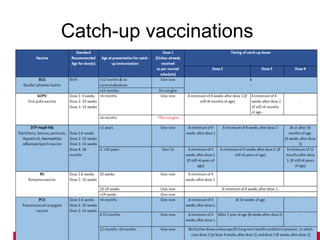
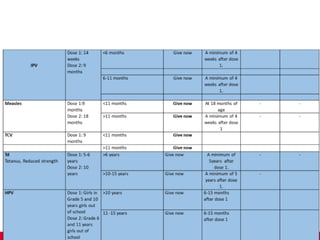
• Catchup vaccines
• New vaccines – Covid19, Ebola etc
#28 Slide 5
Whilst diphtheria typically has a short disease course of a few days, it can last months if complications arise. Diphtheria may also present in a range of clinical manifestations, as described below.1,2
Pharyngeal diphtheria: most common form, abrupt onset with thick membrane covering tonsils, soft palate, oro- and nasopharynx and inflammation of cervical lymph nodes resulting in classical ‘bull-neck’ appearance
Laryngeal diphtheria: occurs in 25% cases, particularly in those under 4 years of age and insidious onset with increasing hoarseness
Mild fever: diagnosis often missed if not accompanied by pharyngeal diphtheria, which may lead to death
Cutaneous diphtheria: indolent skin infection, occurs at wound sites and may act as a source of respiratory infection for others
Other: aural, vaginal and conjuctival diphtheria occur in 2% cases and often secondary to pharyngeal infection.
References
Wharton M, Vitek CR. Diphtheria toxoid. In: Plotkin SA, Orenstein WA, eds. Vaccines. 4th edn. Philadelphia, Saunders: 2004:211–28
2. CDC. Diphtheria. In: Epidemiology and Prevention of Vaccine-Preventable Disease. 8th edn. Atlanta: US Centers for Disease Control and Prevention, 2005:55–64
#30 The anaerobic bacteria are usually introduced into the umbilical stump of newborn babies when cut with unsterile instruments (rasors), or when the wound is dressed with contaminated materials leading to neonatal tetanus.
Affects neural tissue
#35 Slide 9
The incubation period for pertussis is usually between 7–10 days but can last up to 3 weeks.1,2 During this period, Bordetella pertussis invades the mucosa of the nasopharynx, trachea, bronchi and bronchioles. This invasion increases mucus secretion which is initially thin and later becomes viscid. The disease is divided into three distinct stages: catarrhal, paroxysmal and convalescent stages.
During the catarrhal stage, symptoms are often mild and can be indistinguishable from common upper respiratory tract infections such as influenza. Towards the end of this stage, a dry hacking cough develops.2,3
The paroxysmal stage occurs 10–14 days after exposure to B. pertussis and is associated with an increase in the severity and frequency of rapid coughing, which is followed by a hurried, deep inspiration through a partially closed glottis which causes the characteristic ‘whoop’ associated with the disease. Large amounts of viscid mucus are produced, and vomiting, due to the cough or due to gagging on the mucus, is characteristic.
During the convalescent stage, which usually occurs within 2–4 weeks, the coughing and vomiting become less frequent. The coughing may recur for months (‘100-day cough’) and may be exacerbated by subsequent respiratory infections.2,3
References
Linnemann CC Jr. Bordetella. In: Warrell DA, Weatherall DJ, Cox TM, Firth JD, DA eds. Oxford Textbook of Medicine. 4th edn. Oxford, Oxford University Pres: 2003:525–27
2. CDC. Pertussis. In: Epidemiology and Prevention of Vaccine-Preventable Disease. 8th edn. Atlanta: US Centers for Disease Control and Prevention, 2005:75–88
3. Mortimer EA. Pertussis and pertussis vaccine:1990. Adv Pediatr Infect Dis 1990;5:1–33
#36 Slide 10
The most common complications of pertussis are secondary respiratory tract infections such as pneumonia. Other complications, including haemorrhages in the eye, nose bleeds, hernias and physical damage to the lungs, may occur as a result of severe coughing. Central nervous system complications, ranging in severity from minor convulsions to coma and permanent brain damage, may be caused by a lack of oxygen reaching the brain or cerebral haemorrhage occurring as a result of coughing. Complications of the disease can be fatal, the most common causes of death being pneumonia and atelectasis (incomplete expansion of the lung).1,2
The risks of complications and mortality are highest in infants (particularly those under 1 year old) and negligible in children of school age;3 87% deaths occur in infants under 1 year of age.3 The highest reported rates of pertussis-associated hospitalisation (82%), pneumonia (25%), seizures (4%), encephelopathy (1%) and death (1%) occur in infants aged under 2 months.4
References
1. Mortimer EA. Pertussis and pertussis vaccine:1990. Adv Pediatr Infect Diseases 1990;5:1–33
2. CDC. Pertussis. In: Epidemiology and Prevention of Vaccine-Preventable Disease. 8th edn. Atlanta: US Centers for Disease Control and Prevention, 2005:75–88
3. Wortis N, Strebel PM, Wharton M, Bardenheier B, Hardy IR. Pertussis deaths: report of 23 cases in the United States, 1992 and 1993. Pediatrics 1996;97:607–12
4. Farizo KM, Cochi Sl, Zell ER, Brink EW, Wassilak SG, Pariarca PA. Epidemiological features of pertussis in the United States, 1980–89. Clin Infect Dis 1992;14:708–19
#45 NOTE: WHO differs in that only severe immunosuppression is a contra-indication
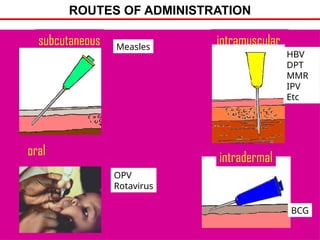
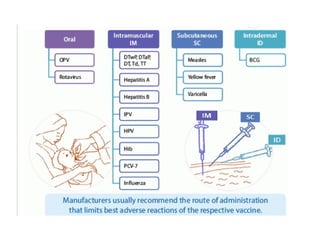
#54 Vaccines are usually given by injection.
Most live-attenuated viral vaccines or non-adjuvanted vaccines are given by the subcutaneous route.
Adjuvanted and sub-unit as well as combined vaccines are generally given intramuscularly. Injections are usually made into the antero-lateral muscle of the thigh in babies and into the deltoid muscle of the upper arm in older subjects. Vaccines should not be injected into the buttocks because then they may be deposited in fat layers which reduces their immunogenicity.
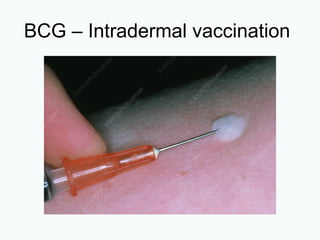
The BCG tuberculosis vaccine is injected intradermally. This route shouldn’t be used for any other vaccines as it is unlikely to provoke an adequate immune response or serious local side effects.
Other ways of administering vaccines are continually being investigated. People who don’t like injections would find orally administered vaccines much more acceptable than injectable vaccines but, to date, the only oral vaccines are the Sabin polio vaccine and a live-attenuated typhoid fever vaccine. Intranasal vaccination may be feasible for some vaccines to prevent respiratory diseases.
Vaccines are never given intravenously. There is a serious risk of a severe reaction if antigens were to be administered directly into the blood stream.
Adrenalin or epinephrine solutions should always be readily available in case of rare anaphylactic reactions.

![IMMUNISATION
• Two FORMS of immunisation
– Passive immunisation
• Natural passive immunisation = transplacental or colostral
transfer of antibodies from the mother to the baby
• Artificial passive immunisation = intramuscular inoculation of
immunolobulin [IG])
– Active immunisation
• Natural - following resolution of natural infection
• Artificial - direct inoculation of a vaccine, the process is called
vaccination
• Important to note that:
– Immunisation is NOT synonymous to vaccination
– Vaccination is another form of immunisation
– Vaccination ONLY involves the use of a vaccine
Science of controlling and preventing infectious diseases](https://image.slidesharecdn.com/vaccination-250423195321-f63e3740/85/Vaccination-program-and-prevention-in-zimbabwe-pptx-19-320.jpg)