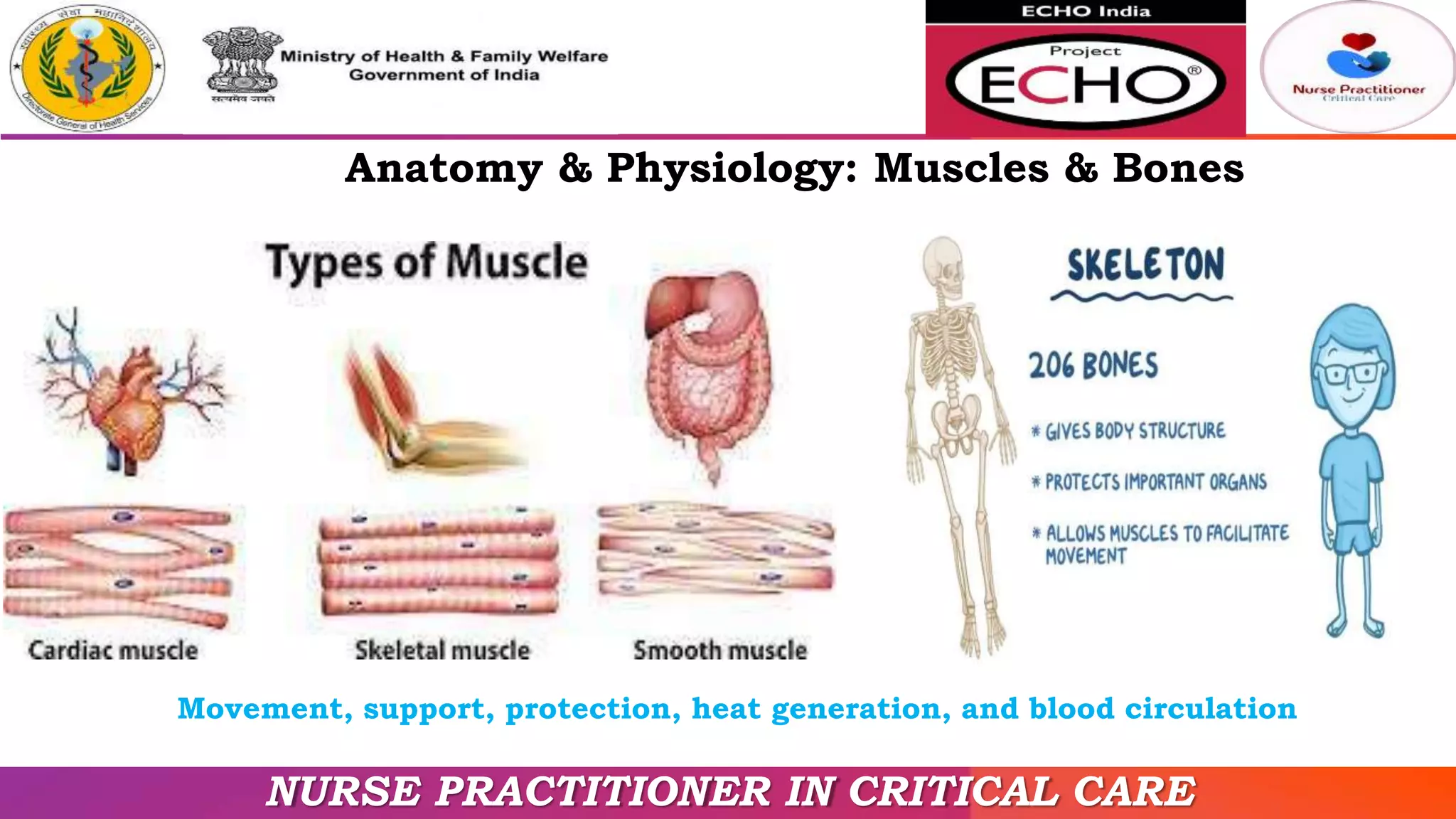
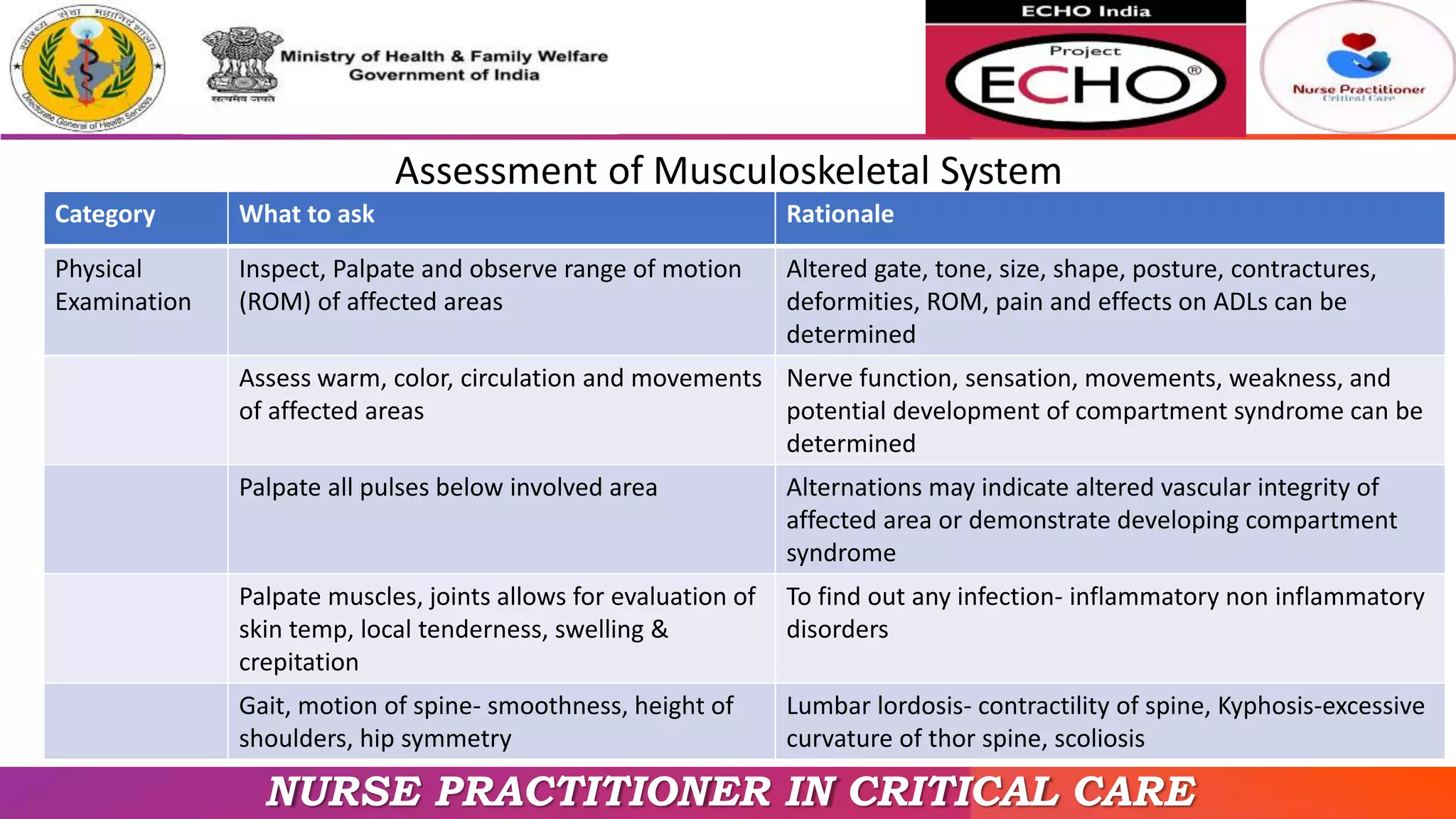
This document provides information on examining the musculoskeletal system. It begins by outlining the objectives of reviewing anatomy and physiology, differentiating normal and abnormal findings, and focused history and physical exam. Various techniques for examining muscles, bones, and joints are described, including inspection, palpation, range of motion tests, and assessing for tenderness, swelling, and deformities. Common musculoskeletal disorders that may be identified during the history and physical exam are also listed. The document aims to equip practitioners to properly examine the musculoskeletal system and identify any potential disorders.



































![Osteomalacia 2nd-150704155942-lva1-app6892 [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/osteomalacia-2nd-150704155942-lva1-app6892autosaved-200520081743-thumbnail.jpg?width=640&height=640&fit=bounds)
































































