1. The Mulligan concept provides pain-free restoration of comfort and mobility through gentle mobilization techniques.
2. It can be used to treat neuromusculoskeletal pain, hypomobility after injuries or surgery, arthritis, and conditions like ankylosing spondylitis. Contraindications include bone diseases, fractures, and certain medical conditions.
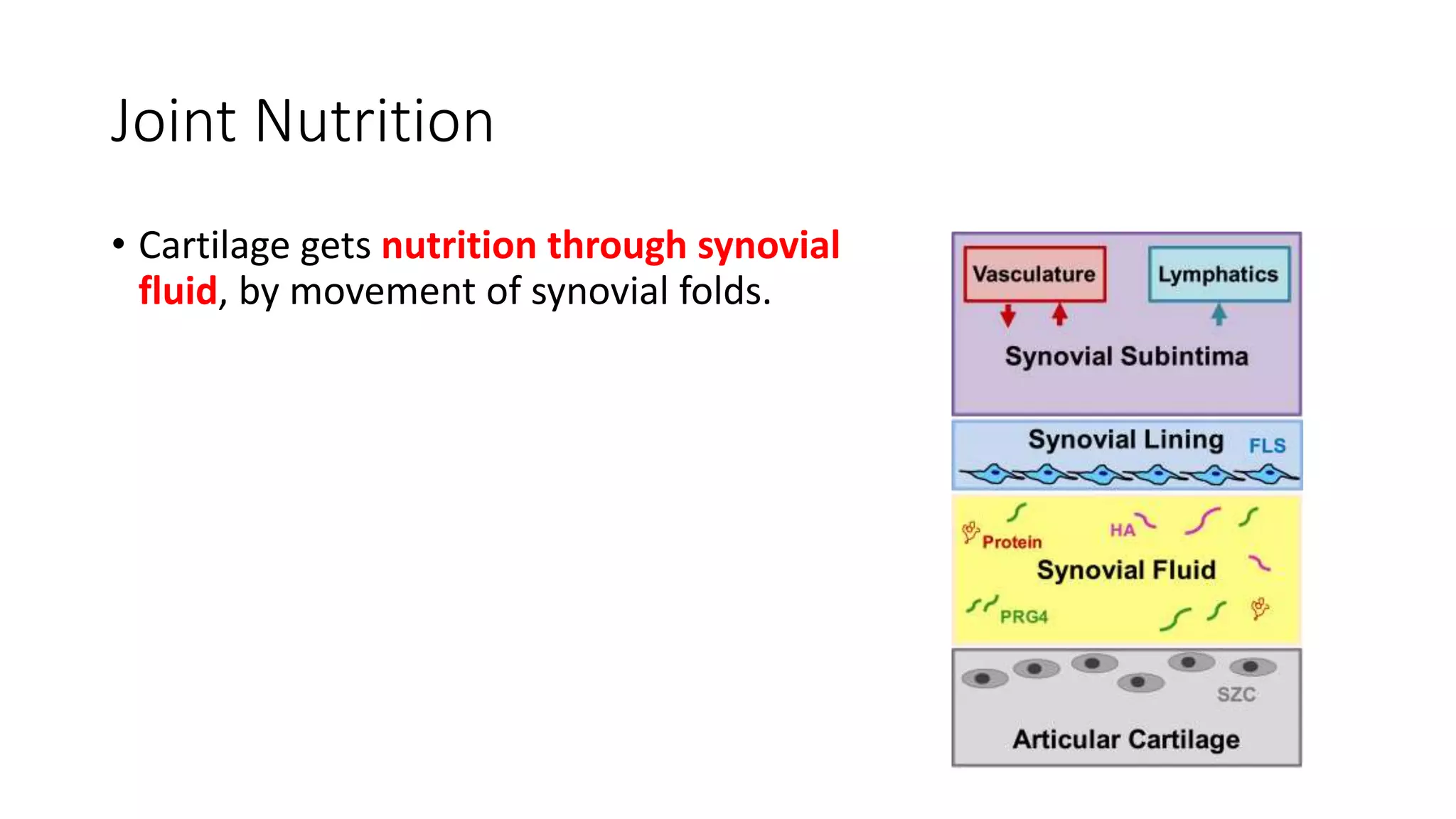
3. The techniques work by stimulating mechanoreceptors in and around the joint to reduce pain and increase range of motion. They also improve joint nutrition and alignment through gentle sustained mobilization in the available range of motion.