Download as PDF, PPTX


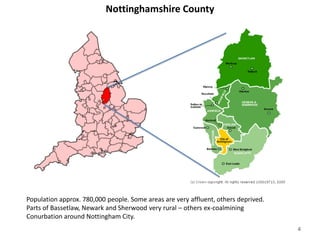
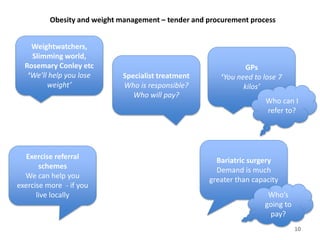
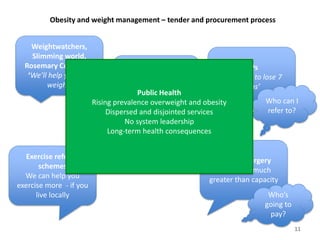

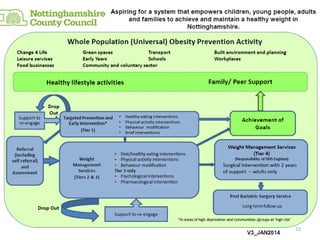
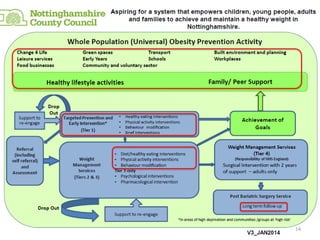
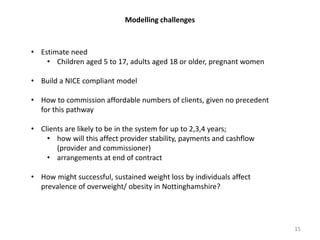
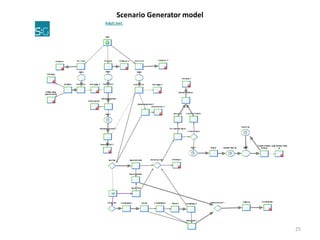
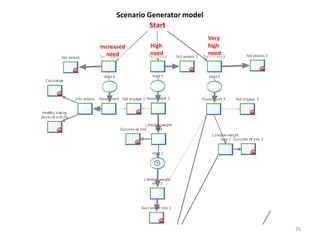
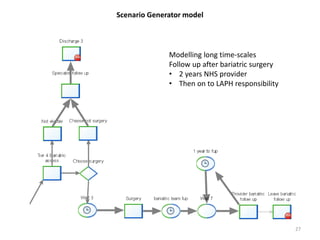
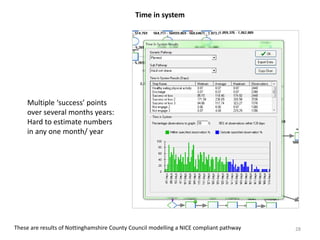
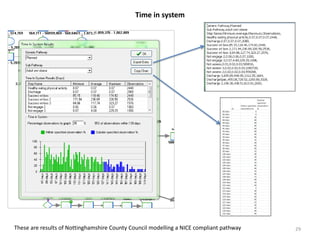
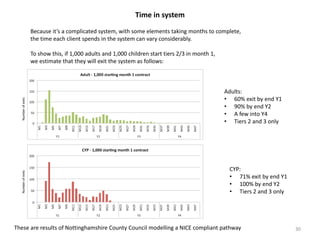
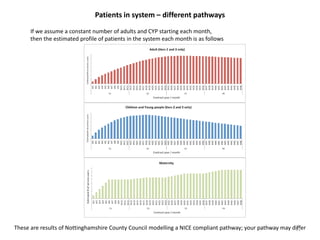
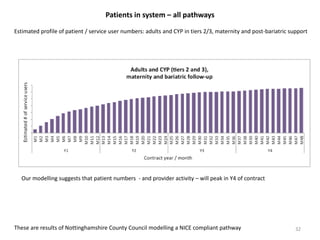

The document outlines an integrated approach to obesity and weight management in Nottinghamshire, detailing challenges in commissioning and modeling under the new local public health structure post-2013. It emphasizes the need for a whole system approach, incorporating various intervention levels and the importance of accurate data modeling to estimate needs and outcomes. The document also highlights the use of a scenario generator for effective modeling of patient pathways and management, ultimately aiming to address the growing prevalence of obesity in the region.































![Presentation 1 ellen_rome[1]](https://cdn.slidesharecdn.com/ss_thumbnails/presentation1ellenrome1-160412185420-thumbnail.jpg?width=640&height=640&fit=bounds)