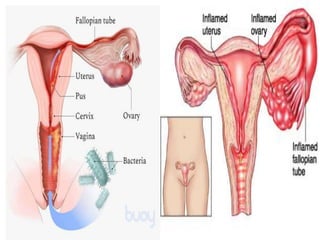
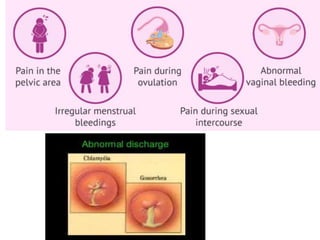
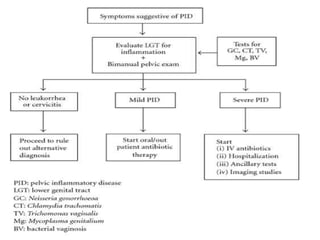
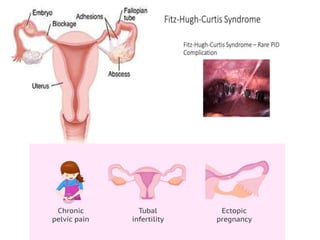
Pelvic inflammatory disease (PID) is an infection of the female upper genital tract that is usually caused by sexually transmitted pathogens like Chlamydia trachomatis and Neisseria gonorrhoeae. It is diagnosed clinically based on symptoms of pelvic or lower abdominal pain along with cervical motion tenderness and can be confirmed with laparoscopy. Treatment involves broad-spectrum antibiotics to cover common causes. Complications include infertility, ectopic pregnancy, and chronic pelvic pain if left untreated. Prevention focuses on sexual health education, screening, and prompt treatment of infections.




















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







