
Download to read offline


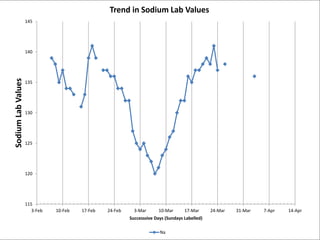
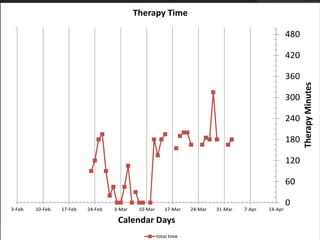
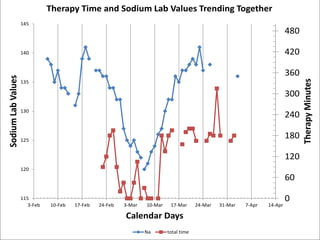
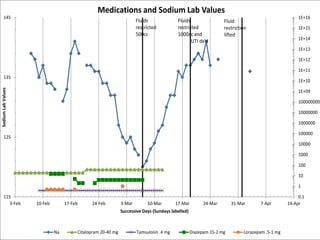
This document discusses using patient behavioral data from rehabilitation records to inform medical treatment. It presents a case study of a patient (Mr. C) whose sodium levels fluctuated and participation in therapy declined as hyponatremia worsened. Correcting the hyponatremia by discontinuing suspected medications (citalopram, tamsulosin) led to improved sodium levels, mood, and greater participation in therapy. The document argues that closely tracking behavioral outcomes can provide insights into medical conditions and responses to interventions that traditional lab tests may miss.














































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


