Download as PDF, PPTX



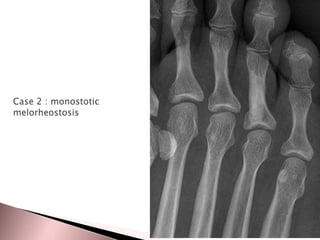





1. Melorheostosis is a rare mesenchymal dysplasia that produces thickened bone with a characteristic dripping wax appearance, most commonly affecting the limbs. 2. It typically presents in childhood and adolescence between ages 5-20 years as limb stiffness or pain. 3. While the condition is usually asymptomatic, when symptoms do occur they include joint stiffness, contractures, pain and limb length discrepancies.



































































