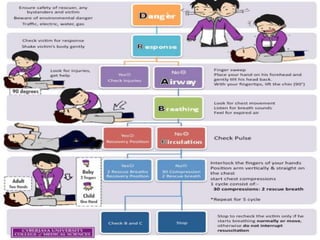
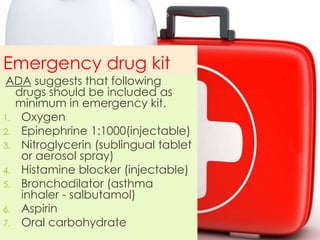
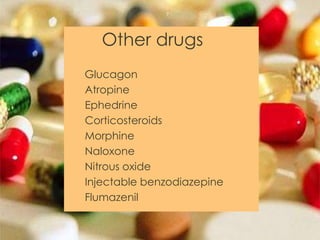
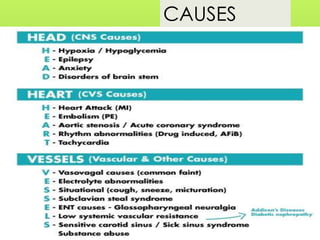
This document provides information on how to manage various medical emergencies that may occur in a dental setting. It discusses approaches to emergencies like syncope, seizures, hypoglycemia, trauma, chest pain, airway obstruction, and asthma. For each emergency, it describes signs and symptoms, prevention strategies, and management steps. The management sections emphasize maintaining the ABCs (airway, breathing, circulation), providing oxygen, treating underlying causes, monitoring vital signs, and seeking definitive medical care as needed. The document also lists common emergency medications and recommends having an emergency drug kit available.































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















