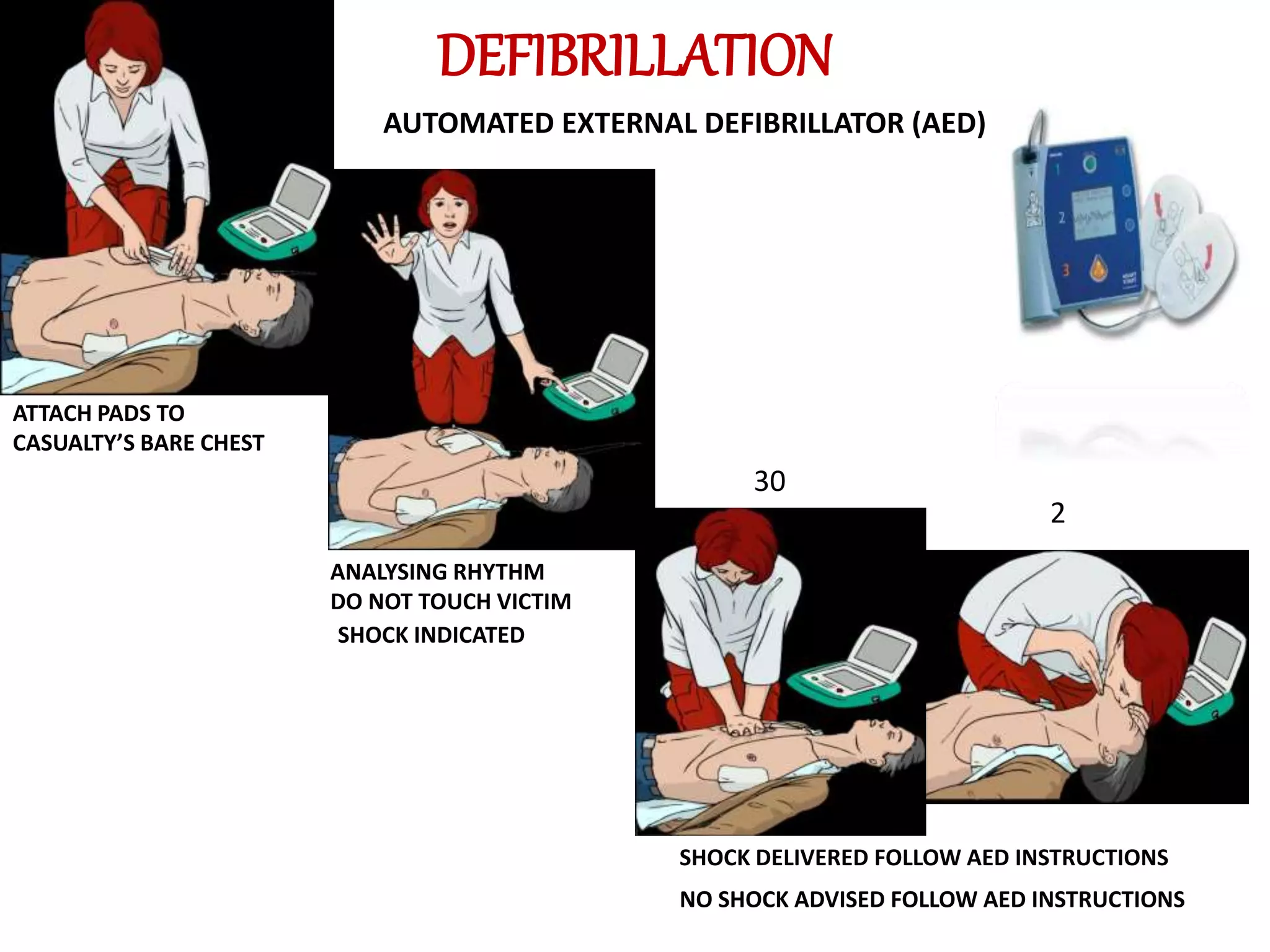
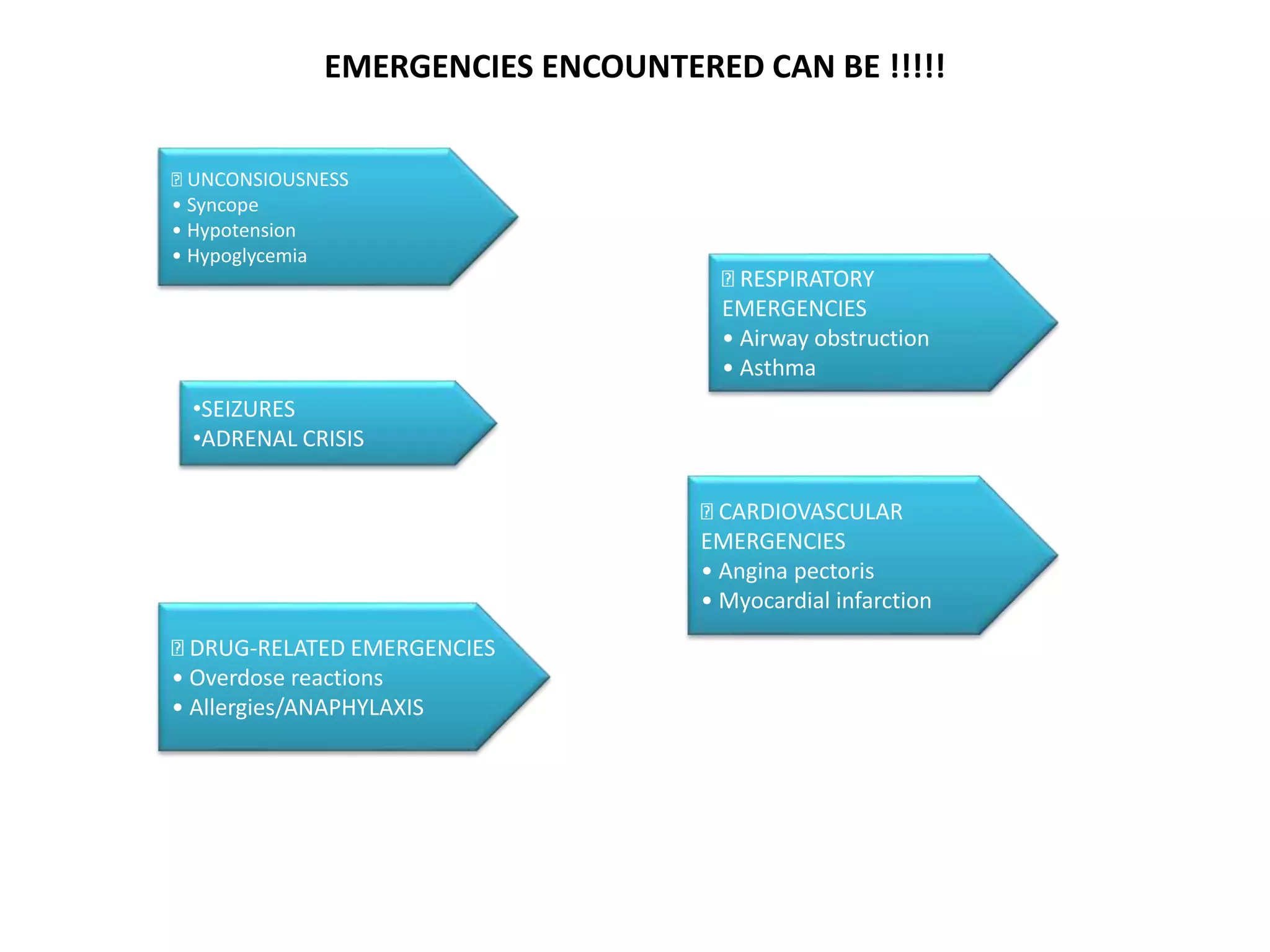
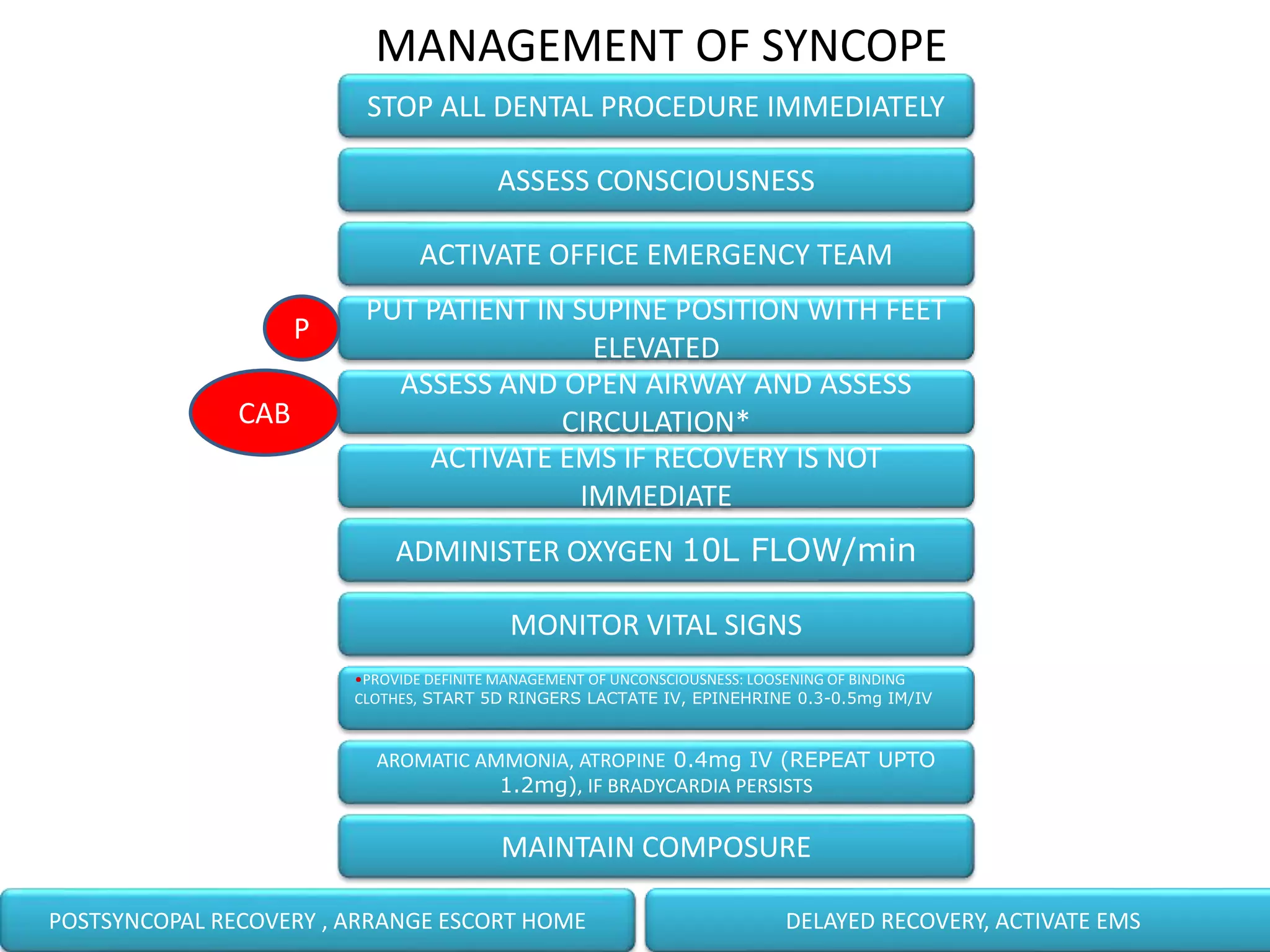
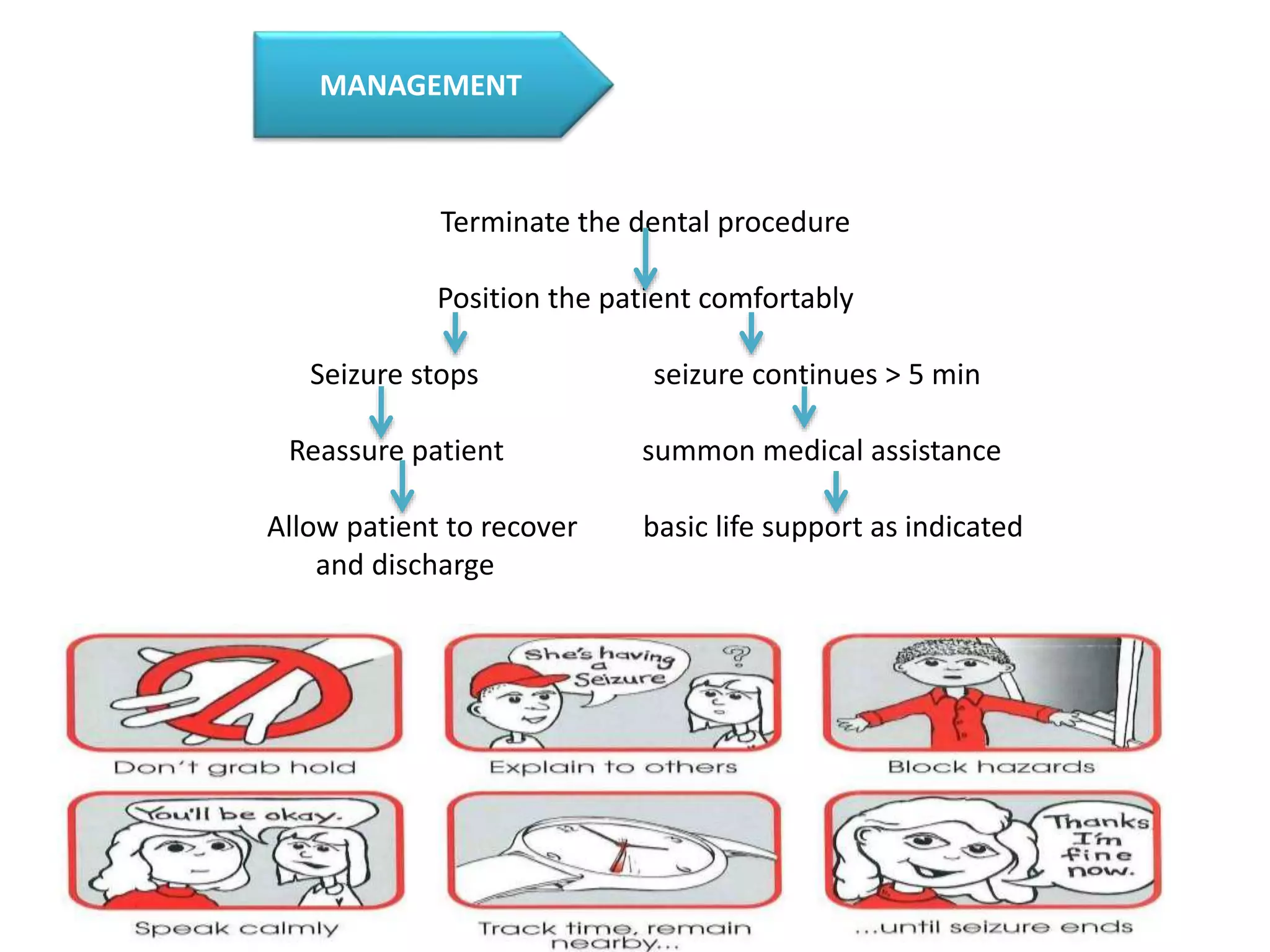
The document outlines essential protocols for managing medical emergencies in dental practice, emphasizing the importance of prevention, preparation, and management. It details various emergencies such as syncope, hypoglycemia, and cardiac arrest, along with recommended treatments and basic life support techniques. The conclusion stresses the need for dental teams to be well-prepared and trained in basic life support to enhance patient outcomes.