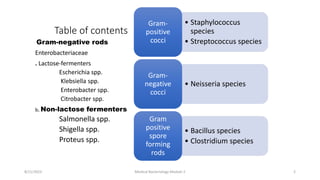
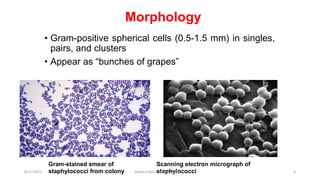
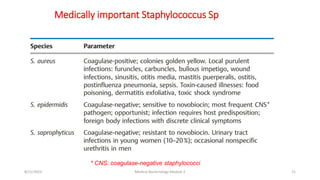
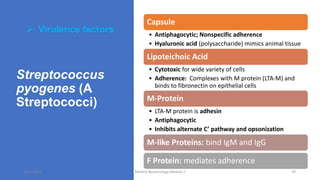
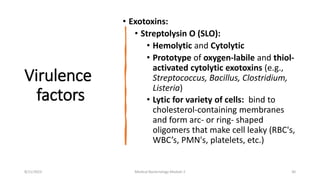
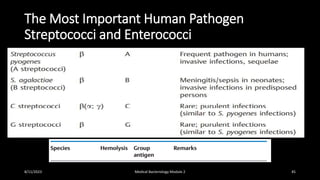
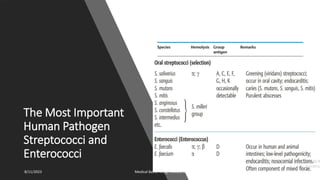
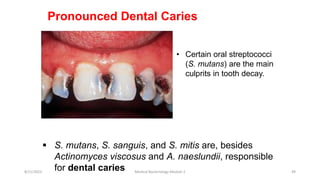
This document provides an overview of medically important bacteria, organized by their characteristics. It discusses Gram-positive cocci like Staphylococcus and Streptococcus species. S. aureus is described as an important pathogen that can cause skin and bloodstream infections. Its virulence factors include toxins and enzymes. Streptococcus species are classified using Lancefield grouping. S. pyogenes is associated with infections like pharyngitis and impetigo, as well as nonsuppurative sequelae such as rheumatic fever. Laboratory diagnosis and treatment options are also summarized.
![Medical
Bacteriology
[Bacteria causing medically important diseases]
8/11/2023 Medical Bacteriology Module 2 1](https://image.slidesharecdn.com/medicalbacteriology-230811135441-6e46a040/85/Medical-Bacteriology-pptx-1-320.jpg)
![Medical
Bacteriology
[Bacteria causing medically important diseases]
8/11/2023 Medical Bacteriology Module 2 1](https://image.slidesharecdn.com/medicalbacteriology-230811135441-6e46a040/75/Medical-Bacteriology-pptx-1-2048.jpg)























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




