Downloaded 67 times


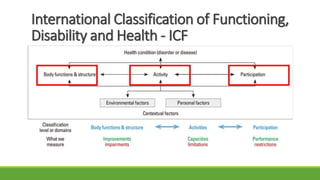

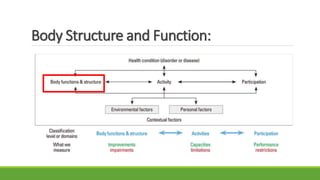



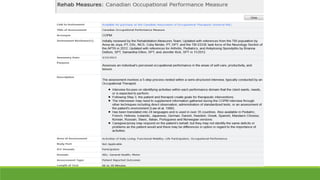










The document discusses new and recently developed measurement tools for occupational and physiotherapists working with school-aged children with motor impairments. It emphasizes the importance of selecting valid and reliable instruments to inform treatment plans, demonstrate outcomes, and promote common language in interventions. Additionally, it reviews various measurement tools categorized into body function and structure, activity, participation, and quality of life, along with resources for accessing these instruments.



































































